Your Testosterone Estrogen Ratio
 Remember those chem lab days. Well, if you do, you may remember that sometimes the concentration of a solvent or chemical is more important than the absolute amount of the same. What I remember even more is getting kicked solidly in the right buttock by my 8th grade chem teacher for goofing around with chemicals in the laboratory, but that's another story.
Remember those chem lab days. Well, if you do, you may remember that sometimes the concentration of a solvent or chemical is more important than the absolute amount of the same. What I remember even more is getting kicked solidly in the right buttock by my 8th grade chem teacher for goofing around with chemicals in the laboratory, but that's another story.
Again, though, the concentration is often critical and this hold true in the hormonal world as well. For example, researchers recently found that it is the ratio of testosterone to estrogen that determines prostate cancer health more than total testosterone.
So what is a good T/E ratio? A solid number for a 20 year old male is 30-40 with some guys shooting near 50. Of course, some would argue that a T/E ratio that high makes it to where most guys can't think straight. Regardless, youthful testosterone-to-estrogen ratios are quite high and are certainly ideal in terms of maintaining male health. A healthy, youthful testosterone/estrogen ratio is about 50:1
Of course, the problem is that guys, as they age, find this all-important testosterone to estrogen ratio steadily decreasing to sometimes even the single digits. The situation seems hopeless because all males find their testosterone simultaneously decreasing and their estrogen increasing. This is assaulting our T/E fraction in both numerator and denominator: you've got the numerator decreasing while the denominator is increasing. Quite the "double whammy", eh?
What causes these rapid changes on both top and bottom in the negative direction. Well, some of it is aging. Males just naturally lose a little testosterone as they age due to mitochondrial dysfunction, DNA and oxidative damage and so on. However, one of the greatest culprits is the extra pounds around our middle. Extra fat pumps out more aromatase which in turn pumps out more estrogen into our system.

 We've heard it over and over again: your diet does not cause acne. However, there are a handful of doctors who believe that what we eat may indeed affect our skin. And they're not pointing fingers at chocolate and potato chips, but instead at milk. That's right -- the wholesome drink that we've always considered healthy is at the center of an acne controversy.
We've heard it over and over again: your diet does not cause acne. However, there are a handful of doctors who believe that what we eat may indeed affect our skin. And they're not pointing fingers at chocolate and potato chips, but instead at milk. That's right -- the wholesome drink that we've always considered healthy is at the center of an acne controversy. DMSO (Dimethyl sulfoxide)
DMSO (Dimethyl sulfoxide)  Carb Cycling.
Carb Cycling. This compound was first manufactured in the early 80’s as an oral tablet, it also comes as an injectable, dragees which are intended for subglossal intake ( Novandrol from Galenika) and as a water dissolved compound (Methyldiol Aqueous).It was widely used by strongman, powerlifters, bodybuilders and lets not forget other bulk users such as wrestlers and foot ballplayers. Even here, users found out that it was beneficial to combine the oral MD with other steroids. After a short period other compounds became more popular and MD seemed to be forgotten. But not in Australia and New Zealand where a lot of veterinary steroids like: Androbol® Denkadiol® Drive® Filybol® Filydoc® Geldabol® Libriol® Metabolin® Methandriol® Metasus® Nandrobolin® Protabol® Spectriol® Superbolin® Tribolin “75” ®, used for animal vetting, contained this magical component. Its purpose here was weight and mass gain. It was very popular in Australia and New Zealand because it was much more easily procured than anabolic/androgenic compounds for human use. Some users claim that MD actually increases cell receptor stimulation, and sensitising the androgenic receptors of the muscle cell and cause other steroids to work better at the site of cell binding. Others claim that it “cleans” the steroid receptors, wich of course is impossible, no such mechanism is known, what it does do is bind very tightly to the steroid binding globules in the blood stream, displacing other, more effective, in the stack added steroids, and possible amplifying them. That is probably why it's included. in some form, in a lot of combination drugs. That is not to say that it is a weak steroid on its own. It certainly is not. Methandriol on itself is a high anabolic, high androgenic steroid. It is used for strength and weight gains. On its own it is highly estrogenic, wich means that it doesn’t need the enzyme aromatase to convert to oestrogen, but it is estrogenic by nature. In a stack or combined steroid cocktail it is only moderate estrogenic. But it is still not very popular on its own. Most products contain methandriol dipropionate in a combined cocktail, only Denkall Mexicana, a vendor of Troy Laboratories from Australia, sells a product that contains only methandriol dipropionate 75mg/ml. This gave US athletes the opportunity to create their own magic. Athletes predisposed to gyno could consider to add Proviron® or Clomid® to their stack as a estrogen blocker. Some lifters feel it works well stacked with injectable testosterones. Actual visible side effects are mild in this drug. The injectable form is only slightly toxic. The most common side effects come from the androgenic portion of the drug and can produce mild acne, oily skin, body and facial hair growth as well as hair loss and high blood pressure. Some report gastrointestinal stress. Overall it's a pretty clean drug in the side effect department.
This compound was first manufactured in the early 80’s as an oral tablet, it also comes as an injectable, dragees which are intended for subglossal intake ( Novandrol from Galenika) and as a water dissolved compound (Methyldiol Aqueous).It was widely used by strongman, powerlifters, bodybuilders and lets not forget other bulk users such as wrestlers and foot ballplayers. Even here, users found out that it was beneficial to combine the oral MD with other steroids. After a short period other compounds became more popular and MD seemed to be forgotten. But not in Australia and New Zealand where a lot of veterinary steroids like: Androbol® Denkadiol® Drive® Filybol® Filydoc® Geldabol® Libriol® Metabolin® Methandriol® Metasus® Nandrobolin® Protabol® Spectriol® Superbolin® Tribolin “75” ®, used for animal vetting, contained this magical component. Its purpose here was weight and mass gain. It was very popular in Australia and New Zealand because it was much more easily procured than anabolic/androgenic compounds for human use. Some users claim that MD actually increases cell receptor stimulation, and sensitising the androgenic receptors of the muscle cell and cause other steroids to work better at the site of cell binding. Others claim that it “cleans” the steroid receptors, wich of course is impossible, no such mechanism is known, what it does do is bind very tightly to the steroid binding globules in the blood stream, displacing other, more effective, in the stack added steroids, and possible amplifying them. That is probably why it's included. in some form, in a lot of combination drugs. That is not to say that it is a weak steroid on its own. It certainly is not. Methandriol on itself is a high anabolic, high androgenic steroid. It is used for strength and weight gains. On its own it is highly estrogenic, wich means that it doesn’t need the enzyme aromatase to convert to oestrogen, but it is estrogenic by nature. In a stack or combined steroid cocktail it is only moderate estrogenic. But it is still not very popular on its own. Most products contain methandriol dipropionate in a combined cocktail, only Denkall Mexicana, a vendor of Troy Laboratories from Australia, sells a product that contains only methandriol dipropionate 75mg/ml. This gave US athletes the opportunity to create their own magic. Athletes predisposed to gyno could consider to add Proviron® or Clomid® to their stack as a estrogen blocker. Some lifters feel it works well stacked with injectable testosterones. Actual visible side effects are mild in this drug. The injectable form is only slightly toxic. The most common side effects come from the androgenic portion of the drug and can produce mild acne, oily skin, body and facial hair growth as well as hair loss and high blood pressure. Some report gastrointestinal stress. Overall it's a pretty clean drug in the side effect department.
 Frequently, athletes research how to better layout an anabolic-androgenic steroid cycle, as well as proper post cycle therapy for making the transition back to a natural training state. Unfortunately, many neglect another component for a successful AAS cycle : maximizing the time spent on using pre-cycle therapy, better know as “priming”
Frequently, athletes research how to better layout an anabolic-androgenic steroid cycle, as well as proper post cycle therapy for making the transition back to a natural training state. Unfortunately, many neglect another component for a successful AAS cycle : maximizing the time spent on using pre-cycle therapy, better know as “priming” Human Chorionic Gonadotropin, or hCG, is perhaps best known as either a fertility drug used to facilitate ovulation, or as an agent used by bodybuilders during or after a cycle of anabolic steroids (AAS) to help maintain or restore testicular function. It is well known that anabolic steroids suppress the hypothalamic-pituitary-testicular axis, preventing testicular Leydig cells from producing the body’s normal complement of testosterone, and leading to what is generally a temporary, reversible testicular shrinkage. The goal of the AAS using athlete or bodybuilder is to bring natural testosterone production back up to normal as quickly as possible after a steroid cycle, so as to maintain strength and size gains made during the cycle, and to avoid sexual dysfunction associated with low testosterone levels.
Human Chorionic Gonadotropin, or hCG, is perhaps best known as either a fertility drug used to facilitate ovulation, or as an agent used by bodybuilders during or after a cycle of anabolic steroids (AAS) to help maintain or restore testicular function. It is well known that anabolic steroids suppress the hypothalamic-pituitary-testicular axis, preventing testicular Leydig cells from producing the body’s normal complement of testosterone, and leading to what is generally a temporary, reversible testicular shrinkage. The goal of the AAS using athlete or bodybuilder is to bring natural testosterone production back up to normal as quickly as possible after a steroid cycle, so as to maintain strength and size gains made during the cycle, and to avoid sexual dysfunction associated with low testosterone levels..jpg) Liver damage is probably the most sensationalized of all possible side effects from oral steroid use. The media often focuses on this particular problem as if it occurs with every steroid, and in every person who takes them. Nothing could be further than the truth. Most anabolic steroids which are ingested orally pass through the liver, which functions as the body´s filtration system. When something goes through the liver, it is broken down by various enzymes, and passed along into the bloodstream. Most research on orally administered anabolic steroids focus on the fact that liver enzymes are elevated following ingestion. But does this necessarily mean that the liver is being damaged, does it? Of course not. All Oral Steroids put stress on the liver. So does alcohol, prescription drugs, asprin and physical conditions lile overweight/obesity.
Liver damage is probably the most sensationalized of all possible side effects from oral steroid use. The media often focuses on this particular problem as if it occurs with every steroid, and in every person who takes them. Nothing could be further than the truth. Most anabolic steroids which are ingested orally pass through the liver, which functions as the body´s filtration system. When something goes through the liver, it is broken down by various enzymes, and passed along into the bloodstream. Most research on orally administered anabolic steroids focus on the fact that liver enzymes are elevated following ingestion. But does this necessarily mean that the liver is being damaged, does it? Of course not. All Oral Steroids put stress on the liver. So does alcohol, prescription drugs, asprin and physical conditions lile overweight/obesity.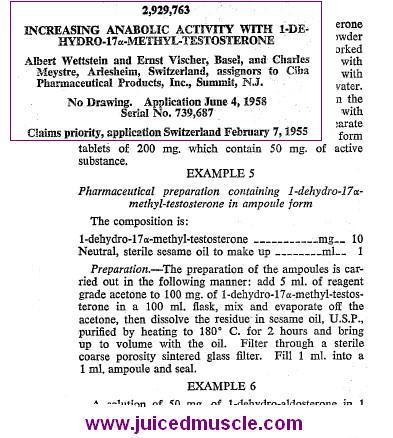 There I also posted this exerpt from the first patent application for 1-dehydrotestosterones which resulted in studies with these new compounds. The scientists from CIBA described a way to manufacture 1 ml ampoules of oil based methandrostenolone for injections. It is pretty obvious that the CIBA scientists studied the results of this new injectable.
There I also posted this exerpt from the first patent application for 1-dehydrotestosterones which resulted in studies with these new compounds. The scientists from CIBA described a way to manufacture 1 ml ampoules of oil based methandrostenolone for injections. It is pretty obvious that the CIBA scientists studied the results of this new injectable.