
Oxandrolone Again

O xandrolone Again
xandrolone Again
You will probably think, why another post about oxandrolone again? One would think that by now everything would be written about this drug. Just like I did in 2015. Not so. Since Oxandrolone is still in use and more and more new applications are tried, also new studies are still published. And because I'm also intrigued by this drug, I tried a less-used application on some older men who want to try this drug as HRT. And not just to restore their hormone levels of QOL (quality of life) but also as a restoration of youthful dynamism, stamina and libido. But also to see if it causes loss of fat mass, and especially of visceral fat. Because this is a long-term in vivo experiment, I will later elaborate with new posts.
 To refreshen your memory: Oxandrolone was first made by Raphael Pappo and Christopher J. Jung while at Searle Laboratories (now part of Pfizer). The researchers first described the chemical in 1962. They were immediately interested in oxandrolone's very weak androgenic effect relative to its anabolic effect It was released as a pharmaceutical drug in the United States in 1964.
To refreshen your memory: Oxandrolone was first made by Raphael Pappo and Christopher J. Jung while at Searle Laboratories (now part of Pfizer). The researchers first described the chemical in 1962. They were immediately interested in oxandrolone's very weak androgenic effect relative to its anabolic effect It was released as a pharmaceutical drug in the United States in 1964.
The drug was prescribed to promote muscle regrowth in disorders which cause involuntary weight loss, and is used as part of treatment for HIV/AIDS. It had also been shown to be partially successful in treating cases of osteoporosis. However, in part due to bad publicity from its illicit use by baseball players, production of Anavar was discontinued by Searle Laboratories in 1989. It was picked up by Bio-Technology General Corporation, which changed its name to Savient Pharmaceuticals who, following successful clinical trials in 1995, released it under the tradename Oxandrin. BTG subsequently won approvals for orphan drug status by the Food and Drug Administration (FDA) for treating alcoholic hepatitis, Turner syndrome, and HIV-induced weight loss. It is also indicated as an offset to protein catabolism caused by long-term administration of corticosteroids.
 Anavar really started to catch on big time with bodybuilders, athletes and recreational steroid users when the publication “Muscle Media 2000” (the first national magazine to talk openly about steroids) in 1996 gave Anavar the highest rating in regard to benefit to risk ratio. Essentially, the magazine told the world that Anavar produced outstanding results with very little toxicity, and the steroid suddenly became one of the most coveted anywhere in the world.
Anavar really started to catch on big time with bodybuilders, athletes and recreational steroid users when the publication “Muscle Media 2000” (the first national magazine to talk openly about steroids) in 1996 gave Anavar the highest rating in regard to benefit to risk ratio. Essentially, the magazine told the world that Anavar produced outstanding results with very little toxicity, and the steroid suddenly became one of the most coveted anywhere in the world.
Read the conclusions of this study, maybe bodybuilders where not so stupid when they decided to use oral steroids to jumpstart their cycles the first 6-8 weeks. Or maybe do several short cycles of this oral. Bad for the liver?
Six-Week Improvements in Muscle Mass and Strength During Androgen Therapy in Older Men Schroeder et al 2005:
Testosterone replacement therapy in older men, even when given for more than a year, has resulted in only modest increases in total lean tissue of 1–2 kg, and the increases in muscle strength have been modest at best and inconsistent. Whereas, treatment with oxandrolone, a p otent oral androgen, produced a robust 3-kg increase in total LBM along with significant increases in appendicular LBM, muscle volume, and maximal voluntary strength of the major muscle groups of the upper and lower body after just 12 weeks of treatment. The only other study in which comparable changes in lean tissue and consistent improvements in the major muscle groups were achieved used largely supraphysiologic doses of testosterone for 6 months.
otent oral androgen, produced a robust 3-kg increase in total LBM along with significant increases in appendicular LBM, muscle volume, and maximal voluntary strength of the major muscle groups of the upper and lower body after just 12 weeks of treatment. The only other study in which comparable changes in lean tissue and consistent improvements in the major muscle groups were achieved used largely supraphysiologic doses of testosterone for 6 months.
Likewise, the FDA-approved dose of oxandrolone (20 mg/ day dose) appeared to be supraphysiologic because endogenous production of luteinizing hormone was suppressed.
Thus, the magnitude of accretion in myofibrillar protein and benefits for skeletal muscle strength may be related to dose or potency of the anabolic androgen used for treatment.
T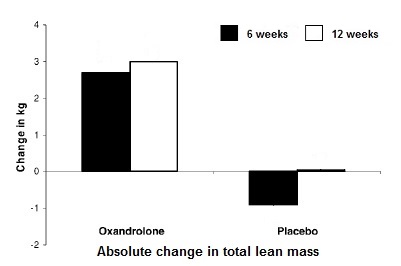 he most important finding of this study was that greater than 90% of the gains in total LBM, appendicular lean tissue, and skeletal muscle strength were achieved by study week 6.
he most important finding of this study was that greater than 90% of the gains in total LBM, appendicular lean tissue, and skeletal muscle strength were achieved by study week 6.
Indeed, total LBM increased by 2.7 ± 1.6 kg at study week 6 and only increased an additional 0.3 ± 0.1 kg by study week 12. Appendicular LBM by DEXA, an indirect measure of muscle mass, increased by 1.2 ± 0.9 kg at study week 6, which was greater than 90% of the gain at study week 12, namely 1.3 ± 0.9 kg. Similarly, the increases in maximum voluntary strength at study week 6 were 93%, 96%, 74%,and 94% of the respective gains for leg press, leg curl, chest press, and lat pull-down at study week 12. These increases in maximal voluntary strength of the upper and lower body appendicular muscles suggest that functionally important improvements may be attained with a relatively short course of therapy using a potent androgen.
T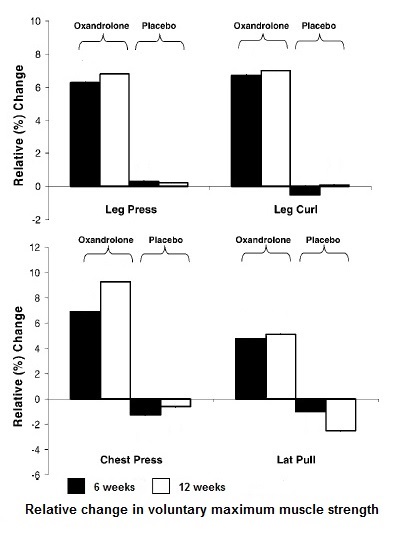 hese observations are consistent with the findings of Bhasin and colleagues, who showed that changes in body composition and skeletal muscle strength are proportional to the dose of testosterone administered for 20 weeks to younger men.
hese observations are consistent with the findings of Bhasin and colleagues, who showed that changes in body composition and skeletal muscle strength are proportional to the dose of testosterone administered for 20 weeks to younger men.
We believe that the significant improvements in maximal skeletal muscle strength corroborate our findings of increased total and appendicular LBM by DEXA scanning and that these findings are not merely the result of hydration from the androgen treatment. Furthermore, our findings of increased thigh muscle volume determined by serial MRI CSA slices support the contention that increases in muscle mass with androgen supplementation are responsible for the gains in strength because CSA is proportional to muscle strength and we have previously shown that increases in muscle CSA are proportional to increases in strength
O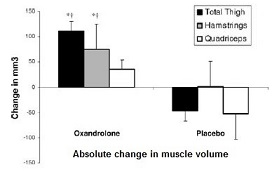 f note, there were greater absolute changes in hamstrings compared to quadriceps muscle volume probably due to the quadriceps muscle compartment being larger and more likely recruited during normal physical activity. The fact that the quadriceps muscle group is more often used for habitual daily activities may explain why this muscle group did not respond as well to the oxandrolone treatment. It is possible that smaller muscle groups, such as the hamstrings, which are not recruited as often for typical patterns of movement or activity, have a lower threshold for stimulus and respond better to androgen therapy.
f note, there were greater absolute changes in hamstrings compared to quadriceps muscle volume probably due to the quadriceps muscle compartment being larger and more likely recruited during normal physical activity. The fact that the quadriceps muscle group is more often used for habitual daily activities may explain why this muscle group did not respond as well to the oxandrolone treatment. It is possible that smaller muscle groups, such as the hamstrings, which are not recruited as often for typical patterns of movement or activity, have a lower threshold for stimulus and respond better to androgen therapy.
Dose Response
What we know now is that even 20 mg is a supraphysiologic doses, but bodybuilders are used to take much bigger doses, Luckily some scientists ran a study to the effect of different doses – 20 – 40 and 80 mg/day. Similar to the eyeopening study of Shalender Bhasin to testosterone, we refer to as the dose response study. And who parcipitated in this study (Oxandrolone in the Treatment of HIV-Associated Weight Loss in Men Grunfeld et al 2006)?
..again our friend Shalender Bhasin.
Administration of oxandrolone has been associated with significant decreases in plasma HDL cholesterol levels and increases in LDL cholesterol levels. The administration of the 40- and 80-mg doses was associated with significant increases in ALT and AST; these increases
were transient and returned toward baseline in most subjects
T he gains in body weight and BCM were related to oxandrolone dose. Similarly, there were dose-dependent increases in AST and ALT levels and common treatment discontinuations attributable to AST and ALT elevations.
he gains in body weight and BCM were related to oxandrolone dose. Similarly, there were dose-dependent increases in AST and ALT levels and common treatment discontinuations attributable to AST and ALT elevations.
Thus, the best trade-off between the anabolic effects and AST and ALT elevation was achieved at the 40-mg daily dose. The therapeutic efficacy and safety of this dose should be further evaluated in subsequent clinical trials.
Oxandrolone treatment was associated with significantly greater body weight gain above baseline than with placebo. A major portion of this weight gain occurred in the lean body compartment, as reflected in the significant gains in BCM, intracellular water, and serum creatinine levels.
The gains in body weight during the double-blind phase of the study were sustained during the open-label phase of the study. Oxandrolone administration has been shown to increase
muscle protein synthesis in emaciated burn patients, muscle mass and maximal voluntary strength in older men at risk for sarcopenia, and weight in patients with cancer cachexia.
Most previous studies have included small numbers of subjects, however; this study is the largest randomized placebo-controlled trial of an androgen in patients with HIV-associated weight loss.
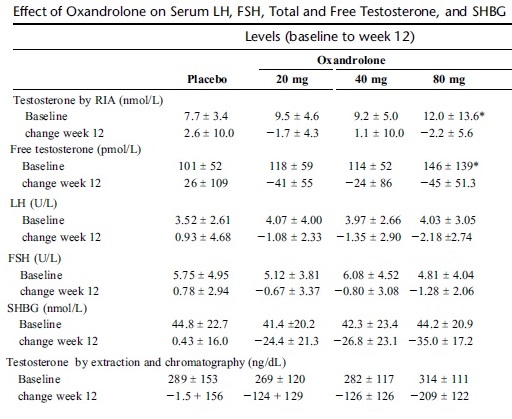
Serum LH and FSH levels decreased significantly during oxandrolone administration, consistent with its androgenic activity. Whereas conventional measurement of testosterone did not show consistent decreases, assay after chromatographic separation did show suppression of testosterone, confirming the androgenic effect and indicating that oxandrolone or a metabolite cross-reacted in the conventional testosterone assay.
This dose-ranging study did not include women; therefore, we cannot determine whether the level of androgenic activity seen with oxandrolone would have the expected detrimental virilizing effects in women.
Oxandrolone administration was generally well tolerated.
Grade III and IV elevations of transaminases were observed in 95% of study participants, however, especially at the 80-mg dose. Careful monitoring of these parameters is therefore indicated after the initiation of oxandrolone therapy. Furthermore, LDL levels increased and HDL levels decreased.
The decreases in HDL and increases in LDL represent a proatherogenic lipoprotein profile. Clinicians therefore need to weigh the risk-benefit ratio of this therapy. Wasting syndrome predicts a significant risk of complications and death, but even studies as large as this one are not large enough and have not been carried out long enough to determine whether reversal of that risk occurs with treatment of wasting and to determine the risk of cardiovascular disease. The risk of atherosclerosis predicted by this lipoprotein profile suggests that such therapy should be restricted to those with significant wasting or should be terminated when wasting has improved. The effects of oxandrolone on HDL cholesterol were not sustained, and 3 months following treatment there was a rebound to levels greater than baseline. Hematocrit levels did not increase in either group. The PSA measures did not change significantly by study week 6; however, by study week 12 there was a small (_0.6 ± 0.9 ng/ml) but significant decrease in the PSA in the oxandrolone group.
Effects of long-term oxandrolone administration in severely burned children. Murphy et al 2004: “Liver transaminases were unaffected. CONCLUSIONS: Long-term administration of oxandrolone safely improves LBM (Lean body mass), BMC (bone mineral content), and BMD (bone mineral density) in severely burned children.”
Treatment with oxandrolone and the durability of effects in older men Schroeder et all 2004: “The course of oxandrolone did not pose health risks. The researchers monitored the men's liver enzymes, cholesterol, LH and the prostate cancer marker PSA, but noticed nothing alarming.”
Now we know oxandrolone is relatively safe to use.
But most bodybuilders just want a hard dense muscular look. So does it work?
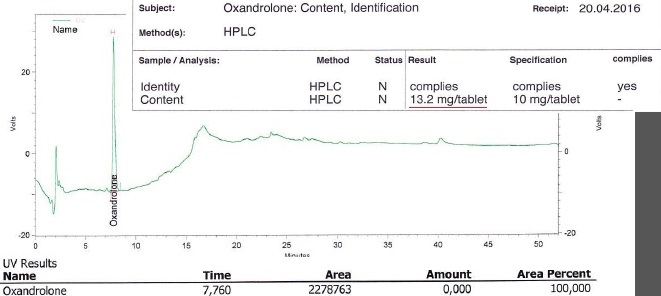
What I wanted to know first was, is it real and is it pure? Because since oxandrolone is very pricey a lot of underground labs cut or substitute their products with cheaper products. As you can see the product is pure and the tabs are even overdosed. So know we know we are experimenting with real oxandrolone at 26.4 mg/day together with 400 mg caffeine that will amplify the strength of the oxandrolone.
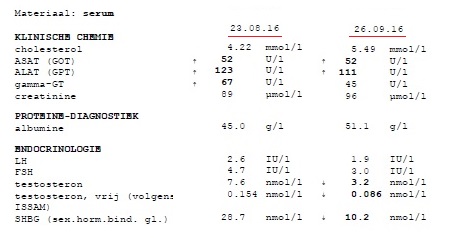
Before starting, one subject had his bloodvalues checked and after 4 weeks he did it again. After PCT he’ll do it again. Since the subjects where older guys with a history of bodybuilding, the oxandrolone/caffeine combo gave quick results, probably also due to muscle memory. Libido after week 3 increased really hard. One guy also had night muscle pumps that kept him awake sometimes. It shows results and sides are very individual. Strength gains are impressive but the subjects stay cautious because an injury is no option. To be continued…

- Login to post comments