
Metribolone-Methyltrienolone-R1881

Metribolone-Methyltrienolone-R1881
 On the left you see a picture of ampoulle made by Newgenpharm, Korea. Its an obvious fake, seen the doses.
On the left you see a picture of ampoulle made by Newgenpharm, Korea. Its an obvious fake, seen the doses.
Metribolone is an extremely powerfull steroid, some experts even call it monstreous. It is hard ro buy the real products and API's. Mostly because its not only extremely potent, but also extremely expensive. Underground manufacturers that don't have direct contact with an manufacturer of these powders and don't have the ability to analyse them will end up with a substitution or a very underdosed product. We all seen that during our analyses and everyone elso know this from the market in recreational drugs. Most recreational drugs (cocaine or speed by example) are cut heavily, because everyone involved wants to make a profit. Believe me there is no difference in Anabolic market.
Underground Labs (UG) now sell this product as designer steroid and also a mixed product (Hard Core Labs MT-DMN) more info at the end of the article.
Labs MT-DMN) more info at the end of the article.
You see in increasing amount of both orals (sold as Oral Tren or Oral Parabolan) aswel as injectables. Scientific research showed that subQ injected "oral steroids" where a minimum tenfold more potent then the oral version.
On the rigt you see a picture with UG Labs selling more realistic dosed products. Geneza Pharma with 250mcg/tab. Genpharm with 10 mg/ml and DutchLabs with 2 mg/ml
In the area of pro-hormones there was a methyldienolone product on the supplement market. That of course disapeared with all other pro-hormones.
Methyltrienolone is essentially the same compound as trenbolone that has gone under 17 alpha alkylation so that it can remain active after oral administration. So in a basic sense, methyltrienolone offers all of the advantages of trenbolone with the added bonus of being orally active. However, that extra benefit comes with a hefty price when it comes to hepatoxicity as will be demonstrated below.
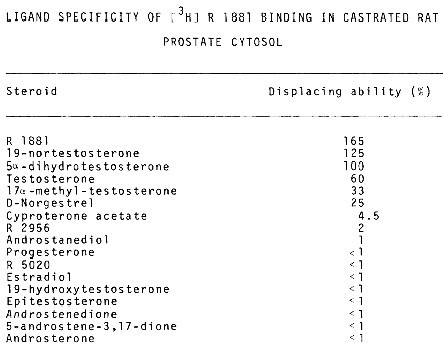
Like trenbolone methyltrienolone has an extremely strong binding affinity for the androgen receptor as well, even surpassing that of testosterone. This of course supports the assertion that trenbolone is extremely anabolic as by binding to the androgen receptor a compound is able to activate the anabolic mechanisms that are dependent upon the androgen receptor, one of the many ways that anabolic steroids aid muscle growth. Androgen receptors also exist in adipose tissue. When stimulated by way of a compound such as methyltrienolone binding to them, this can result in a higher then normal lipolytic action (1). So not only does this drug help to build muscle, it can help to burn fat.
Another rather unique characteristic of methyltrienolone is its anti-catabolic abilities. Methyltrienolone binds with the receptors that interact with glucocorticoid hormones, these being catabolic hormones (2). By being able to inhibit cortisol and some other catabolic hormones in the body methyltrienolone is ideal for those users that are attempting to reduce body fat as the compound will help to minimize muscle wasting when running a calorie deficit.
Use/Dosing
 Methyltrienolone was originally developed by a French pharmaceutical company, but never commercially produced due to its severe hepatoxic effects. That should indicate how truly harsh this drug is. For this reason it is important that users use caution when dosing this drug and ensure that they keep their cycles of it to brief periods of time. This would also include the exclusion of other steroids that are overly hepatoxic, such as 17 alpha alkylated oral steroids.
Methyltrienolone was originally developed by a French pharmaceutical company, but never commercially produced due to its severe hepatoxic effects. That should indicate how truly harsh this drug is. For this reason it is important that users use caution when dosing this drug and ensure that they keep their cycles of it to brief periods of time. This would also include the exclusion of other steroids that are overly hepatoxic, such as 17 alpha alkylated oral steroids.
In terms of cycle duration, four weeks is the standard length that most users limit themselves too if not shorter. Any extension of this time would absolutely necessitate continuous blood tests conducted by a doctor, something that is a good idea no matter how long a user intends to run this drug. Of course, individual response to the drug and the liver function of a user would also factor into how well a user is able to tolerate methyltrienolone and thereby run the drug.
As for dosing, since little research has been conducted using methyltrienolone since its first production we are left to use anecdotal information to determine exactly how much of the compound one should administer to see its benefits as well as limiting the side effects. Doses ranging from 400-800 micrograms for male users are quite normal for most. Females are not recommended to administer this drug, as will be discussed in the section below. Of course like all drugs doses much higher then these have been run. This also has led to a much higher reporting rate of negative side effects, including temporary liver conditions such as jaundice. For this reason it is recommended that users remain quite careful whenever initially dosing this compound, as well as any increases that they may make.
Risks/Side Effects
Similar to trenbolone, methyltrienolone does not exhibit any estrogenic activity and therefore estrogenic side effects are not a concern with this compound itself. It is also resistant to the 5 alpha reductase enzyme, but this is of little comfort to a user as methyltrienolone is already of the most androgenic drugs in common use by steroid users. For this reason androgenic side effects should be expected by most users that undertake a cycle of this drug. Prostate enlargement and oily skin/acne are commonly reported by users. The effect of the drug on the hair of the user should also close to that of trenbolone. Anecdotally many users have reported that trenbolone is one of, if not the, harshest compound for losing one's hair. The same can be said of methyltrienolone. If a user is genetically predisposed to male pattern baldness he may want to avoid this compound.
Having listed the harsh androgenic nature and side effects associated with methyltrienolone, it should come as no surpirse that women are not recommended to use this compound. The usual virilizing effects such as deepening of the voice, body/facial hair growth, and enlargement of the clitoris, among others are likely to cause problems for female users. These effects can appear at even relatively low doses as has been proven in animal studies (3). Methyltrienolone is not a compound that women should attempt to administer.
Now due to the lack of estrogenic side effects associated with methyltrienolone it would seem that users would have little to worry about in terms of side effects like gynecomastia, water retention, etc. However one again like trenbolone, methyltrienolone is a progestin, meaning that it has the ability to bind to receptors of the female sex hormone progesterone (4). Also, like other 19-nor compounds methyltrienolone increases prolactin levels. Side effects related to these reactions can include breast growth and lactation. The drug also has the ability to help enhance any estrogenic side effects that may results from aromatizing drugs that the user is administering concurrently. This is obviously something to take into consideration when deciding what ancillary drugs to use during a cycle that includes methyltrienolone. To prevent side effects as they relate to increased prolactin levels a user can use several compounds including bromocriptine, vitamin b6, and/or cabergoline. Letrozole can also be used to lower progesterone levels.
Being a progestin, methyltrienolone also has a dramatic effect on users’ natural testosterone production. Much in the same way that trenbolone and nandrolone do, methyltrienolone can suppress the natural production of testosterone for an extended period of time. For this reason it is advisable that users use testosterone in conjunction with methyltrienolone even during short cycles if they wish to avoid sexual dysfunction, libido problems, or mental side effects associated with a lack of testosterone. There have been some animal studies that have shown that methyltrienolone can actually increase libido in some cases (5), but others have found the opposite effect to be true as well (6). As a precautionary measure, testosterone supplementation may be a good protocol to follow.
As stated earlier in this profile, methyltrienolone was deemed to be to hepatoxic for commercial human use by the company that originally developed it. As a 17 alpha alkylated steroid, it would be assumed that the drug would put an additional strain on the liver of a user. However it seems that methyltrienolone is one of the harsher steroids in terms of hepatoxicity. For this reason, it can be expected that the liver values of a user will become elevated if he or she uses methyltrienolone for any moderate period of time. In fact liver damage could be a significant risk if doses or durations of cycling the drug range outside of excepted standards of if the user has any liver abnormalities. For this reason using other 17 alpha alkylated steroids at the same time as methyltrienolone, or even relatively close to the same time as the drug, is considered to a risk that one should not endeavour to take.
Doping
Steroid experts William Llewellyn and Patrick Arnold have each called methyltrienolone one of the “most powerful” anabolic steroids ever created. It is also one of the most hepatotoxic androgens ever produced. Initially developed by Roussell-UCLAF during the 1960s, the hepatoxicity of Metribolone prevented its commercial release. Bill Roberts likened the toxicity of methyltrienolone to that of taking high dosages of Anadrol combined with high dosages of Halotestin concurrently. As you can clearly see by te bloodvalues as posted in the article on MT-DMN the administration of Metribolone subQ avoids the " first pass" through the liver and this way of usage avoids to much stress on the liver.
According to Patrick Arnold, some athletes used methyltrienolone in the 1990s and smoothly passed doping controls searching methyltrienolone because of the very small quantities of the steroid required for performance enhancing effects. He was somewhat surprised that methyltrienolone was detected by drug testers in the Greek steroid scandal showing that anti-doping tests have improved for the substance; 11 Greek weighlifters and 4 Greek track and field athletes tested positive for methyltrienolone prior to the 2008 Beijing Olympic Games.
 A mixed product containing 3 mg/ml Metribolone (MT) and 200 Di-Methyl-Nandrolone (DMN).
A mixed product containing 3 mg/ml Metribolone (MT) and 200 Di-Methyl-Nandrolone (DMN).
This UG Lab also sells a 10 mg/ml MT product and a separate DMN product.
We covered MT-DMN here:
//juicedmuscle.net/content/blood-values-theoretical-vs-practical-blood-values
The data posted below are from oral use of Metribolone. As we can see in the bloodvalues from MT-DMN usage (link) injectable administration of Metribolone differs greatly from oral use.
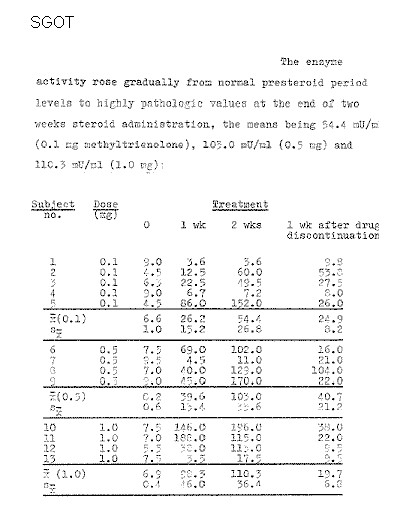
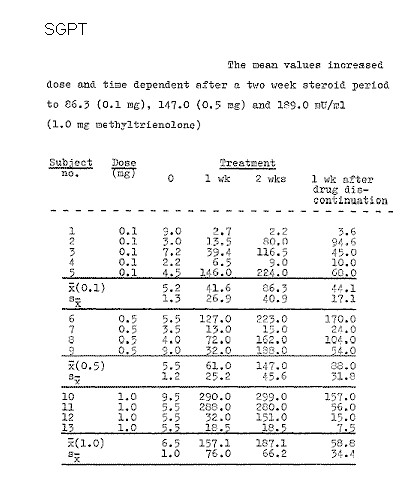
German researchers (1) published in 1966 an experiment in which they admistrated small doses of metribolone to 13 subjects for two weeks. The doses ranged from 0.1 milligrams to 1 milligram per day. This slight dose proved sufficient from earlier trials to to increase protein build up.
This light dose already caused liver problems, discovered the Germans when they investigated a number of levels in the blood of their subjects. The concentrations of glutamate-pyruvate transaminases - short GPT - and glutamate-oxalacetate-transaminases - GOT - grew explosively. Normally, these values remain within the 5.12 milli-units per milliliter.
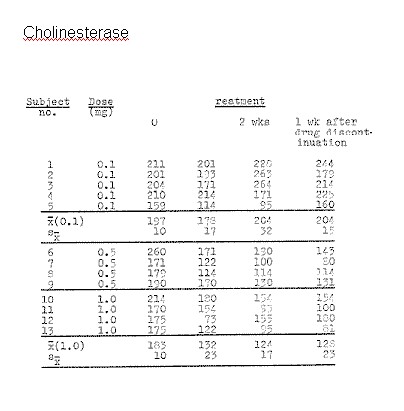
Less dramatic was what happened with the concentration of the enzyme cholinesterase. In the group receiving 1 milligram per day the concentration decreased. And restored when the cycle of two weeks was over, nothing more.
The researchers found more defects, but they were smaller. Their conclusion was that the new steroid was downright dangerous. Despite the extremely light dose the subjects had side effects resembling a poisoning with the carcinogen Carbon-tetrachloride. Methyltrenbolone was the most toxic steroid made until now
Later researchers would use Metribolone, of which one milligram per day could already disrupt the liver, for research. Then they also discovered methyltrienolone was leading the list of androgenic means that could cause prostate cancer.(2) ( R1881 is the same as methyltren).
References
1. Sjogren J, Li M, Bjorntorp P. Androgen hormone binding to adipose tissue in rats. Biochim Biophys Acta. 1995 May 11;1244(1):117-20.
2. Ho-Kim MA, Tremblay RR, Dube JY. Binding of methyltrienolone to glucocorticoid receptors in rat muscle cytosol. Endocrinology. 1981 Nov;109(5):1418-23.
3. Lax ER, Baumann P, Schriefers H. Changes in the activities of microsomal enzymes involved in hepatic steroid metabolism in the rat after administration of androgenic, estrogenic, progestational, anabolic and catatoxic steroids. Biochem Pharmacol. 1984 Apr 15;33(8):1235-41.
4Dube JY, Tremblay RR, Chapdelaine P. Binding of methyltrienolone to various androgen-dependent and androgen-responsive tissues in four animal species. Horm Res. 1976;7(6):333-40.
5. Sodersten P, Gustafsson JA. Activation of sexual behaviour in castrated rats with the synthetic androgen 17 beta-hydroxy-17 alpha-methyl-estra-4,9,11-triene-3-one (R 1881). J Endocrinol. 1980 Nov;87(2):279-83.
6.Baum MJ, Kingsbury PA, Erskine MS. Failure of the synthetic androgen 17 beta-hydroxy-17 alpha-methyl-estra-4,9,11-triene-3-one (methyltrienolone, R1881) to duplicate the activational effect of testosterone on mating in castrated male rats. J Endocrinol. 1987 Apr;113(1):15-20.
7.USATODAY.com. 2008. "Eleven Greek weightlifters test positive; coach suspended".
Pharmaceutical Name: Methyltrienolone
Chemical Structure: 17beta-Hydroxy-17-methylestra-4,9,11-trien-3-one
Chemical Formula: C19H24O2
Molecular Weight: 284.3974
Active Life: four to six hours
Anabolic/Androgenic Ratio: approximately 12 000/6 000
- Login to post comments