
Tamoxifen for Bodybuilders Good or Bad?


Recently Nolvadex (tamoxifen) has become a bad reputation, especially since some moderators and discussionboard members copy paste articles, that contain alarming percentages about high decreases in IGF-1 and free testosterone after tamoxifen usage. This coupled with spectacular increases in adipose tissue.
But is that true? What we know is that Old School bodybuilders used Nolvadex and Clomid during their cycle and in the PCT. Thus is tamoxifen aka nolva that bad? Let’s take a closer look.
Tamoxifen Citrate (Nolvadex) is an antagonist of the estrogen receptor in breast tissue. It has been the standard endocrine (anti-estrogen) therapy for hormone-positive early breast cancer, although aromatase inhibitors have been proposed for postmenopausal women. Some breast cancer cells require estrogen to grow. Estrogen binds to and activates the estrogen receptor in these cells. Tamoxifen is metabolized into compounds that also bind to the estrogen receptor but do not activate it. Furthermore tamoxifen prevents estrogen from binding to its receptor. Hence breast cancer cell growth is blocked. Bodybuilders use tamoxifen as an effective drug to prevent gynecomastia (gyno). A daily dose of 20mg is already enough.
Gynecomastia: Clinical evaluation and management Cuhaci et al 2014 :
“Gynecomastia is the benign enlargement of male breast glandular tissue and is the most common breast condition in males. At least 30% of males will be affected during their life. The prevalence of gynecomastia was reported to be between 32-65%, due to use of different methods of assessment and the analysis of males of different ages and with different lifestyles, while autopsy data suggest a prevalence of 40%
Because gynecomastia causes anxiety, psychosocial discomfort and a fear of breast cancer, patients seek medical attention and require diagnostic evaluation. Because of the increasing incidence of obesity, the number of patients with pseudo-gynecomastia is increasing. In addition, increased use of anabolic steroids and environmental contamination with xenoestrogens or estrogen-like substances may stimulate glandular proliferation in male breast tissue”
Tamoxifen is not only very suitable in preventing gynecomastia, it can also be used to reverse an already existing gyno, a remarkable study in that regard was performed by Devoto et al 2007:
“Forty three patients with gynecomastia, aged 12 to 62 years, were studied. Twenty seven patients had a pubertal physiological gynecomastia, in eight it was caused by medications, in four it was secondary to hypogonadism, in three it was idiopathic and in one it was due to toxic exposure. Twenty patients had mastodynia and in 33, gynecomastia had a diameter over 4 cm. It lasted less than two years in 30 patients, more than two years in nine and four did not recall its duration. All were treated with tamoxifen 20 mg/day for 6 months. A follow up evaluation was performed at three and six months of treatment.”
“ RESULTS: Mastodynia (painful sensitivity of the breast and nipple) disappeared in all patients at three months. At six months gynecomastia disappeared in 26 patients (62%), but relapsed in 27%. All gynecomastia’s caused by drugs with anti-androgen activity disappeared. Fifty two percent of gynecomastias over 4 cm and 90% of those of less than 4 cm in diameter disappeared. Fifty six percent of gynecomasti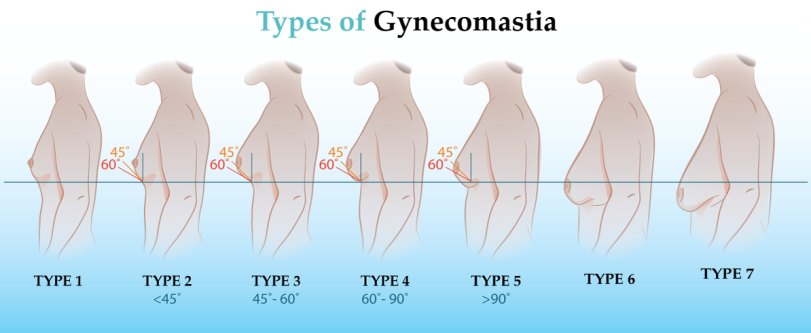 as lasting more than two years and 70% of those of a shorter duration disappeared.” “CONCLUSIONS: Tamoxifen is safe and effective for the treatment of gynecomastia. Larger lesions have a lower response to treatment.”
as lasting more than two years and 70% of those of a shorter duration disappeared.” “CONCLUSIONS: Tamoxifen is safe and effective for the treatment of gynecomastia. Larger lesions have a lower response to treatment.”
So much for all kinds of gynecomastia’s originated for different reasons and existing for different length of years.
From an article on the net:
Negatives Of Tamoxifen Use
A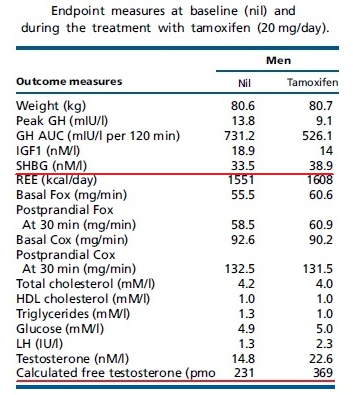 lthough classed as an estrogen antagonist it should be noted that in some parts of the body tamoxifen actually acts as an estrogen agonist meaning it actually acts in an estrogenic manner as opposed to how most think of it being which is an anti-estrogen. When it acts in an estrogenic fashion in the liver for instance, tamoxifen can increase levels of sex hormone binding globulin (SHGB) which acts to bind to testosterone thus lowering free testosterone in the body. Free testosterone is the amount of unbound testosterone in the system and it is the level of free testosterone which is strongly correlated to the positive effects of high testosterone such as increased muscle mass, strength, and libido. By lowering free testosterone, tamoxifen has the potential to hurt our bodybuilding gains. This helps to explain why we never hear of people using tamoxifen on a standalone basis (similar to how a testosterone booster is used) and gaining any muscle mass despite the significant rise in testosterone it is capable of producing. Quite simply, a lot of the testosterone rise is cancelled out by the increase in SHGB. Is that true? The numbers of the quoted study show that tamoxifen not only increases SHGB (a bit), but at the same time increases LH and thus testosterone and the net result is more Free T.
lthough classed as an estrogen antagonist it should be noted that in some parts of the body tamoxifen actually acts as an estrogen agonist meaning it actually acts in an estrogenic manner as opposed to how most think of it being which is an anti-estrogen. When it acts in an estrogenic fashion in the liver for instance, tamoxifen can increase levels of sex hormone binding globulin (SHGB) which acts to bind to testosterone thus lowering free testosterone in the body. Free testosterone is the amount of unbound testosterone in the system and it is the level of free testosterone which is strongly correlated to the positive effects of high testosterone such as increased muscle mass, strength, and libido. By lowering free testosterone, tamoxifen has the potential to hurt our bodybuilding gains. This helps to explain why we never hear of people using tamoxifen on a standalone basis (similar to how a testosterone booster is used) and gaining any muscle mass despite the significant rise in testosterone it is capable of producing. Quite simply, a lot of the testosterone rise is cancelled out by the increase in SHGB. Is that true? The numbers of the quoted study show that tamoxifen not only increases SHGB (a bit), but at the same time increases LH and thus testosterone and the net result is more Free T.
A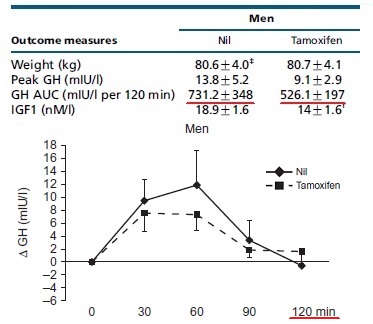 nother negative of tamoxifen's action in the liver is its ability to suppress production of the peptide hormone IGF-1. IGF-1 is broken down from growth hormone and is considered to be more potent than growth hormone itself for the purposes of building muscle tissue. High IGF-1 levels make a big contribution to the process of building a better physique and the ability of tamoxifen to suppress IGF-1 levels is another reason why tamoxifen use tends to be disappointing for the purposes of building muscle mass.
nother negative of tamoxifen's action in the liver is its ability to suppress production of the peptide hormone IGF-1. IGF-1 is broken down from growth hormone and is considered to be more potent than growth hormone itself for the purposes of building muscle tissue. High IGF-1 levels make a big contribution to the process of building a better physique and the ability of tamoxifen to suppress IGF-1 levels is another reason why tamoxifen use tends to be disappointing for the purposes of building muscle mass.
I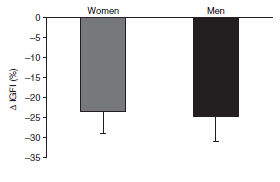 n fact, a recent study which showed a rise in total testosterone (they failed to measure free testosterone or levels of SHGB) and a reduction in IGF-1 levels after tamoxifen usage is a significant indicator as to why it can prove disappointing for the building or maintenance of muscle mass. The fact that tamoxifen is referred to as an anti-estrogen overlooks the fact that outside of certain tissues it promotes estrogenic effects. GH was stimulated with an infusion of 30 grams of L-arginine hydrochloride over a 30 min period. Blood samples for GH level measurements were taken at baseline and 30, 60, 90 and 120 min after commencement of arginine infusion. The same goes for IGF-1. What is the relevance, if you would use tamoxifen in PCT, what bodybuilders do for decades, and if you would inject GH or IGF-1 or secratogogues during PCT the results should be blunted a bit. Natural bodybuilders don’t use tamoxifen, but hard core bodybuilders after a heavy cycle to maintain gains, not to gain musclemass.
n fact, a recent study which showed a rise in total testosterone (they failed to measure free testosterone or levels of SHGB) and a reduction in IGF-1 levels after tamoxifen usage is a significant indicator as to why it can prove disappointing for the building or maintenance of muscle mass. The fact that tamoxifen is referred to as an anti-estrogen overlooks the fact that outside of certain tissues it promotes estrogenic effects. GH was stimulated with an infusion of 30 grams of L-arginine hydrochloride over a 30 min period. Blood samples for GH level measurements were taken at baseline and 30, 60, 90 and 120 min after commencement of arginine infusion. The same goes for IGF-1. What is the relevance, if you would use tamoxifen in PCT, what bodybuilders do for decades, and if you would inject GH or IGF-1 or secratogogues during PCT the results should be blunted a bit. Natural bodybuilders don’t use tamoxifen, but hard core bodybuilders after a heavy cycle to maintain gains, not to gain musclemass.
A study published in the Journal of Endocrinology(3) showed that long term tamoxifen use increased serum testosterone levels by 50% which is certainly a healthy increase. However, at the same time serum estrogen levels increased by a massive 341%. In fact, in the control group in this study, which only used tamoxifen for a week, estrogen rose after just four days. Considering that the subjects in this trial used tamoxifen at a lower dose of just 10mg it begs the question of what would happen if used at the higher dose typically seen in bodybuilding circles. These numbers are taken from the study from Willis KJ et al : Hormonal effects of tamoxifen in Oligospermic men. Percentages from studies on oligospermic men cannot be extrapolated to normal men, and short time effects do not indicate that these effects stay the same during prolonged use. Also tamoxifen usage results are very gender specific and highly intra-individual.
Hormonal effects of an antiestrogen, tamoxifen, in normal and oligospermic men.
Vermeulen et al 1978:
“The administration of tamoxifen, 20 mg/day for 10 days, to normal males produced a moderate increase in luteinizing hormone (LH), follicle-stimulating hormone (FSH), testosterone, and estradiol levels, comparable to the effect of 150 mg of clomiphene citrate (Clomid). Treatment of patients with "idiopathic" oligospermia for 6 to 9 months resulted in a significant increase in gonadotropin, testosterone, and estradiol levels.
However, whereas Clomid produced a decrease in the LH response to LH-releasing hormone (LHRH), no such effect was seen after the administration of tamoxifen. In fact, prolonged treatment (6 weeks) with tamoxifen significantly increased the LH response to LHRL.”
Improving the elasticity of the blood vessels
Bodybuilders taht tamoxifen may also be making their blood vessels more healthy, and reducing their risk of a fatal heart attack. We deduce this from a trial done by researchers in Cambridge, England.
T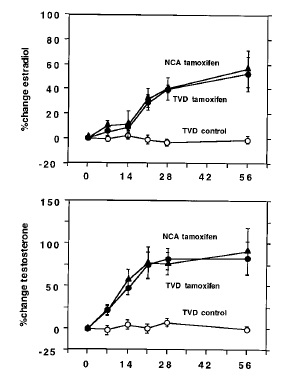 amoxifen is the active ingredient in Nolvadex. Tamoxifen is a SERM: a compound that is capable of attaching itself to the receptor for the female sex hormone estradiol. What's more, tamoxifen is an anti-oestrogen. The compound forces estradiol off its receptor, thereby preventing estradiol from doing its work. Tamoxifen then sits in the estradiol receptor a bit like a key that has broken off in a lock. No other key can be put in the lock, but the door won't open either. Athletes use tamoxifen to counter the side effects of oestrogens, which are produced when testosterone is converted into estradiol. Tamoxifen is also used after taking a course of steroids to boost the body's own testosterone production.
amoxifen is the active ingredient in Nolvadex. Tamoxifen is a SERM: a compound that is capable of attaching itself to the receptor for the female sex hormone estradiol. What's more, tamoxifen is an anti-oestrogen. The compound forces estradiol off its receptor, thereby preventing estradiol from doing its work. Tamoxifen then sits in the estradiol receptor a bit like a key that has broken off in a lock. No other key can be put in the lock, but the door won't open either. Athletes use tamoxifen to counter the side effects of oestrogens, which are produced when testosterone is converted into estradiol. Tamoxifen is also used after taking a course of steroids to boost the body's own testosterone production.
In the British study, 30 men with furred up arteries were given 40 mg of tamoxifen every day for 56 days. The researchers wanted to know more about the effect of tamoxifen on the heart and the blood vessels. Estradiol has good and bad effects on the heart and arteries. It increases the amount of 'good cholesterol' HDL, which is positive. But it also causes blood clots, which is not such good news.
The men's testosterone levels rose, and their estradiol levels rose too. Apparently the conversion of testosterone into estradiol simply c ontinued.
ontinued.
NCA = 10 male patients with a history of chest pain suggestive of angina pectoris but with normal coronary angiograms. TVD = men with a triple-vessel disease, i.e. clogged up arteries in the heart. This group was given statins and aspirin.
The researchers used a complicated procedure to measure the elasticity of the men's blood vessels [ED-FMD]. In the graph on the right you can see that the tamoxifen treatment increased the elasticity.
If you're healthy and under 40, then you probably have an ED-FMD of 7 percent. As you get older your ED-FMD declines to around 5 percent by the age of 51. At your ED-FMD is 3.5 percent. The NCA group had an average age of 51. The average age of the TVD group was 63. So the cardiovascular age of the men decreased.
 The graphic on the left shows more cardiovascular parameters.
The graphic on the left shows more cardiovascular parameters.
Most effects are favourable. Lipoprotein (a) is a building block of the 'bad' LDL cholesterol. The more of this you have in your blood, the more worried the cardiologists get. The lower the amount of triglycerides and LDL in your blood, the better. They both have an adverse effect on the HDL.
All in all, the researchers were pleasantly surprised by the results of their research. "The data provide strong evidence to support clinical evaluation of SERMs for the treatment of men with CAD", they write in the last sentence of their article.
Visual problems?
Tamoxifen is acutely toxic to the eyes with more than one report on a bodybuilding forum showing a user who irreversibly damaged their eyesight.
Tamoxifen-associated eye disease. A review. Nayfeld et al 1998
Case reports and case series identify crystalline retinal deposits, macular edema, and corneal changes as potential tamoxifen ocular toxicities. Extensive retinal lesions and macular edema with visual impairment have been reported in a few patients receiving high-dose tamoxifen. Less extensive retinal changes may occur in patients receiving low doses for long periods, and isolated retinal crystals may be observed in patients without visual symptoms. Conclusion: Ocular toxicity is uncommon in the current clinical setting of long-term, low-dose tamoxifen use.
Are there better options then Tamoxifen?
Neuroendocrine Regulation of Growth Hormone and Androgen Axes by Selective Estrogen Receptor Modulators in Healthy Men. Birzniece et al 2009
Ten healthy men were randomized to 2-wk sequential treatment with tamoxifen (10 and 20 mg/d) and raloxifene (60 and 120 mg/d), with a 2-wk intervening washout period. Main Outcome Measures: We measured the GH response to arginine and circulating levels of IGF-I, LH, FSH, testosterone, and SHBG. Results: Tamoxifen, but not raloxifene, significantly reduced IGF-I levels by 25 ± 6% and increased SHBG levels by 20 ± 7% at the higher therapeutic dose. There was a nonstatistically significant trend toward a reduction in the GH response to arginine with both SERMs. Both drugs significantly increased LH, FSH, and testosterone concentrations.
The mean increase in testosterone 40 vs. 25% and LH 70 vs. 30% was significantly greater with tamoxifen than with raloxifene treatment.
Conclusions: Tamoxifen, but not raloxifene, reduces IGF-I levels. Both SERMs stimulate the gonadal axis, with tamoxifen imparting a greater effect. We conclude that in therapeutic doses, raloxifene perturbs the GH and gonadal axes to a lesser degree than tamoxifen.
Tsourdi et al 2009:
Tamoxifen, raloxifene and toremifene are SERMs: they dock to the receptor for estradiol but don't start up the processes that usually follow after estradiol has docked itself to its receptor. That's why doctors use SERMS against tumors whose growth is stimulated by female hormones.
B odybuilders use SERMs because they raise the testosterone level. One of the ways that the body monitors its own production of sex hormones is by keeping an eye on the concentration of estradiol in the blood. If it gets too high then sex hormone production is reduced – including the production of testosterone. Because the control mechanisms make use of estradiol receptors, SERMs crank up testosterone production. That’s why bodybuilders use substances like tamoxifen after taking a cycle of steroids.
odybuilders use SERMs because they raise the testosterone level. One of the ways that the body monitors its own production of sex hormones is by keeping an eye on the concentration of estradiol in the blood. If it gets too high then sex hormone production is reduced – including the production of testosterone. Because the control mechanisms make use of estradiol receptors, SERMs crank up testosterone production. That’s why bodybuilders use substances like tamoxifen after taking a cycle of steroids.
The Greek researchers did a trial with just under three hundred infertile men, whose sperm count was low and most of whom had low levels of testosterone production. The researchers gave the men either 20 mg tamoxifen, 60 mg toremifene or 60 mg raloxifene daily for three months. The table above shows what happened to the men's LH, FSH and testosterone levels.
R aloxifene has little effect on the testosterone level, so it's not an interesting candidate for a Post Cycle Therapy supplement. Toremifene is somewhat better, but doesn't perform as well as tamoxifen, and it loses its maximum effect after two months as well.
aloxifene has little effect on the testosterone level, so it's not an interesting candidate for a Post Cycle Therapy supplement. Toremifene is somewhat better, but doesn't perform as well as tamoxifen, and it loses its maximum effect after two months as well.
To complete the story we've added the table left, which shows the effect of the three on sperm cells. Once again, raloxifene performs less well than tamoxifen and toremifene.
The researchers suspect that the two more effective SERMs not only work through the body's hormonal thermostat, thereby inducing the pituitary gland to make more messenger hormones [which in turn get the testes to produce more testosterone]. They think that tamoxifen and toremifene also have a direct effect on the testosterone producing cells.
T amoxifen improves blood lipid ratio
amoxifen improves blood lipid ratio
Dnistrian et al 1993: The effect of tamoxifen on serum cholesterol, high density lipoprotein cholesterol (HDL-cholesterol), low density lipoprotein cholesterol (LDL-cholesterol) and the ratio of LDL-cholesterol to HDL-cholesterol (LDL-C/HDL-C) was investigated in breast cancer patients undergoing therapy for advanced disease. Longitudinal studies in 24 patients treated with tamoxifen (10 mg, twice daily) indicated average decreases in total serum cholesterol (17%) and LDL-cholesterol (27%), whereas the effect of tamoxifen on HDL-cholesterol varied with the individual patient. There was a significant decrease in the LDL-C/HDL-C ratio (33%) consistent with a decreased risk for coronary artery disease. This beneficial influence of tamoxifen on risk factors associated with cardiovascular disease was evident in both premenopausal and postmenopausal patients whether tamoxifen was administered alone or in combination with cytotoxic chemotherapy.
Nóvoa et al 2002: The estrogenic actions of tamoxifen on lipid profiles and hemostasis have been extensively demonstrated in women. That’s why they decided to study healthy boys with pubertal gynecomastia who were given 10 mg tamoxifen per day.
Total cholesterol and lipoprotein(a) showed moderate but significant decreases from baseline. Low-density lipoprotein and high-density lipoprotein cholesterol concentrations as well as triglyceride and apolipoprotein B levels became lower, but these changes were not statistically significant. Among clotting parameters, antithrombin III was reduced, and von Willebrand factor increased significantly. Markers of activated coagulation and fibrinolysis remained unchanged throughout the period of therapy.
The effects of tamoxifen on blood lipids and hemostasis we found in this group of healthy young men were qualitatively similar, but lesser than those previously described in women.
…and protects bones.. Schopman et al: Twelve men with infertility and low-normal serum levels of testosterone were studied before and during tamoxifen therapy. Increases in the serum levels of LH, FSH, testosterone and calcitonin were observed after treatment. Our findings suggest that testosterone has a direct influence on calcitonin secretion.
Calcitonin has a bone sparing effect. Because calcitonin ensures the absorption of calcium from the blood to the bones, the bones become stronger. This reduces the chance of getting osteoporosis.
Imbalance
Finally, the use of aromatising products should be limited and if these are going to be used an AI as opposed to an SERM is a much better solution for managing estrogen levels on cycle. For those who insist on using tamoxifen during PCT it is important this is combined with an AI to help mitigate against the prospect of rebound gyno which could potentially occur with tamoxifen use.
Cakan et al 2009: It was the aim of this study to investigate the effect of a low testosterone/estradiol (T/E2) ratio and the normalization of this ratio by an aromatase inhibitor, anastrozole, on the treatment results of tamoxifen citrate (TAM) in idiopathic oligoasthenoteratozoospermic patients with a normal T/E2 ratio.
Results: A significant decrease in the T/E2 ratio was seen in the majority of the patients during tamoxifen treatment. Normalization of this ratio by addition of anastrozole to the treatment regimen improved the treatment outcomes. However, a placebo-controlled study is needed to confirm our results.
Finally can we use a small dose of testosterone with tamoxifen?
Adamopoulos et al 1997 evaluated the effects of combined tamoxifen citrate and testosterone undecanoate treatment on seminal parameters in men with idiopathic oligozoospermia.
Eighty oligozoospermic men were randomized to receive placebo, T undecanoate (40 mg three times per day), tamoxifen citrate (10 mg two times per day), or T undecanoate plus tamoxifen citrate.
I n the bottom row you can see that the combination of Andriol and tamoxifen not only results in a higher testosterone level, but also in more FSH. So it is possible: to take androgens and at the same time stimulate the pituitary and the testes to produce more testosterone
n the bottom row you can see that the combination of Andriol and tamoxifen not only results in a higher testosterone level, but also in more FSH. So it is possible: to take androgens and at the same time stimulate the pituitary and the testes to produce more testosterone
.When a cycle of steroids is taken the testes usually shrink in size. But during this trial the volume of the testes actually increased. The men also produced more sperm as a result of the treatment, and the combination of Andriol and tamoxifen was most effective.
Now, an oral dose of 120 mg of testosterone-undecanoate is of little interest to bodybuilders. But maybe it's also possible to keep the axis up if instead of taking Andriol you take a more effective anabolic steroid, that places relatively little pressure on the axis. Say, stanozolol, mesterolone or oxandrolone.
