
Performance-enhancing drugs and teen athletes

 Young athletes see and read news stories about famous athletes, artists and celebrities, who admit to having used performance-enhancing drugs. So it's no surprise that as many as 1 in 20 teenagers reports using steroids to increase muscle mass.
Young athletes see and read news stories about famous athletes, artists and celebrities, who admit to having used performance-enhancing drugs. So it's no surprise that as many as 1 in 20 teenagers reports using steroids to increase muscle mass.
Adolescents use a wide variety of drugs and supplements, including anabolic steroids, to improve their sports performance and physical appearance. Prevalence rates for steroid use generally range between 4% and 12% for male adolescents and between 0.5% and 2% for female adolescents. Steroid use among U.S. teens has been on the rise since the early 1990s, but some groups of teens are using more than others. In 1993, one in 45 high school students admitted to using anabolic steroids.
By 1999, the number increased to one in 27. Today, one in 16 high school students, about 1.5 million, admit to using PEDS. The numbers do not include teens taking nutritional supplements laced with steroids or steroid precursors like androstenedione. But let’s keep realistic, it’s not safe in all cases, but I think may other substances cause a bigger threat to the health of young people. Talking about Marihuana, alcohol, cigarettes, prescription drugs abuse, XTC, speed etc. But I don’t close my eyes for the fact that many young people abuse all kinds of different substances at the same time. But I’m sure you would like to read about roids.
According to a new study of anabolic-androgenic steroid (AAS) abuse based on sexual preferences, gay male teens use steroids at a rate six times higher than their straight counterparts. The study authors don’t provide a clear explanation for the disparity in steroid use between gay and straight male teens, but health experts have a few theories. Some say gay teens are more likely to be bullied in school, and that their steroid use becomes a way to protect themselves. Others suggest gay teens are more concerned with physical appearance than straight teens. Researchers speculate gay male adolescents take steroids as an extreme way to look more attractive. Generally speaking, the gay male subculture places a greater emphasis on physical appearance than straight men do. Originally bodybuilding originates from gay guys starting to build a better looking body. In those years bodybuilding was seen as a gay practice. Nowadays we can’t imagine it, but people really thought swole muscles where useless, and bodybuilders where big but not really strong. That changed when Arnold won stone-lifting in Munich.
Nowadays bodybuilding is influenced differently than a few decades back. In those years the most important source of information where the bodybuilding magazines. Bodybuilding back than was revolving around lies. Lies that only served one purpose and that purpose was, selling as much as possible, worthless supplements to young bodybuilders. Now social media and especially YouTube showing Bostin Loyd telling you all about his way of bodybuilding. And all about the dark secrets such as insulin and Synthol. So long Weider liars.
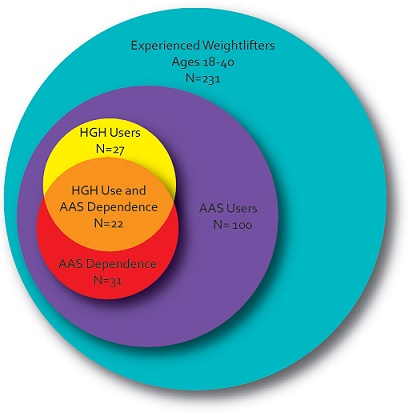
 In 2010 study of performance-enhancing substance use among 231 experienced young male weightlifters, was found that 27 (12%) reported illicit use of human growth hormone (HGH) or its bioactive derivative, insulin-like growth factor-1 (IGF-I). All of these 27 men also reported use of anabolic-androgenic steroids (AAS) and 22 (81%) met criteria for current or past AAS dependence. Fifteen (56%) also reported current or past dependence on opioids, cocaine, and/or ecstasy. These findings suggest that among young male weightlifters, illicit HGH use has become a common form of substance abuse, frequently associated with both AAS dependence and classical substance dependence
In 2010 study of performance-enhancing substance use among 231 experienced young male weightlifters, was found that 27 (12%) reported illicit use of human growth hormone (HGH) or its bioactive derivative, insulin-like growth factor-1 (IGF-I). All of these 27 men also reported use of anabolic-androgenic steroids (AAS) and 22 (81%) met criteria for current or past AAS dependence. Fifteen (56%) also reported current or past dependence on opioids, cocaine, and/or ecstasy. These findings suggest that among young male weightlifters, illicit HGH use has become a common form of substance abuse, frequently associated with both AAS dependence and classical substance dependence
Although the short-term health effects of anabolic steroids, such as effects on the liver, serum lipid levels, the reproductive and cardiovascular systems, and moods and behavior, have been increasingly studied, the long-term health effects are not well known. Steroid users are more likely to be male, participate in strength-related sports, and use other drugs. The effects of many other potential risk factors have not been fully elucidated, however. Assessment of anabolic steroid abuse includes physical, mental status, and laboratory examinations. Steroid cessation, supportive therapy, and adjunctive pharmacotherapies are all employed in treating steroid abuse and dependence. Case studies of anabolic steroid use by females and males are presented
Though most commonly seen in bodybuilding, AAS are also prevalent in non-bodybuilder circles when there is dissatisfaction with one’s physique, a desire to shed unwanted fat, or the need to gain additional muscle mass. Many teenagers seek chemical assistance in fulfilling social and athletic goals. According to the Monitoring the Future Survey by The University of Michigan, in 2006, 2.7% of high school seniors reported they had tried steroids at least once in their lifetime. The majority of those who fall victim to teenage steroid abuse are male athletes seeking to better their performance in sports, be more competitive in the pursuit of athletic scholarships, or to gain recognition outside of the arena. Females as well as males have shockingly admitted trying steroids as early as age 11, and are said to most commonly do so for aesthetic purposes. The charted and graphical illustrations below demonstrate some of the trends seen over the past several years. Some scientists said many steroid users suffer from muscle dysmorphia, a disorder in which people believe their muscular build is undersized, which in return causes them to desire bigger muscles

On the pics: New rising Russian star Aleksej Lesukov and his friend Andrey Skoromnyy, who live the successful bodybuilding life many young bodybuilders dream about. What they have in common with other bodybuilding celebrities is the fact that they started young and where determent to reach their goal.
Let’s not forget that Arnold started juicing at 15 years of age, he used Dianabol which was completely legal in those years and no one had any knowledge about the dangers. We call it genetics, but maybe, just maybe it might be the combination.
I always see in Aleksej a young Lee Priest. And maybe they are both overlooked due to their height.
Abuse or Addiction?
Abuse is different from addiction, and will always precede it in drug use. This earlier incidence is why abuse is the more easily treatable and curable of the two. Drug abuse begins when one has made the decision to use repeatedly, and if used too often drugs create associated physiological cravings within the body. Another characteristic of drug use is that of hindered brain functioning. Neurotransmitters are messengers within the brain that signal the rest of the body to feel and act. Drug use literally alters brain chemistry to the extent that these messages cannot be properly relayed. The continued disruption of these messages causes compulsive drug cravings, that if unaltered result in addiction. Though not every user becomes an addict, this behavior is especially dangerous in adolescents whose young brains and bodies are still developing. For this demographic permanent side effects are likely to occur.
Addiction involves two basic things: (1) Drug seeking behavior – taking large amounts of time finding, buying and then using steroids, and; (2) Dependence – The loss of the ability to stop using the drug, a period in which the body becomes so accustomed to the drug that it is required to function. Some signs that a teenager may be addicted are: a loss of control over the amount used, which is often much more than originally intended; preoccupation with steroid use and body image; continued use despite knowledge of risks and negative effects; the development of tolerance; a need for higher dosages to achieve prior effects; continued use as an avoidance of withdrawal symptoms; disruption normal daily activities; declining grades; and withdrawal from normal school and social functioning.
Sudden cessation of AAS use without some form of step down therapy can be dangerous and possibly result in physical withdrawal symptoms. These are often seen when a parent or coach has found and confiscated the AAS and include cravings, fatigue, depression, restlessness, decreased appetite, insomnia, headaches and decreased interest in sex.
A new study shows that about five percent of middle and high school students have used anabolic steroids to put on muscle, and that as many as one-third of boys and one-fifth of girls have used protein powder or shakes. Between five and 10 percent admitted to using non-steroid muscle-enhancing substances like creatine.
Many kids see steroids as a tool to speed up the process of achieving their ideal body type and enhancing their athletic performance. And of course, this keeps them preoccupied with an image that they feel the need to achieve at any cost.
Anabolic steroids can cause many side effects, in both genders, side effects caused by anabolic steroids include, heart attack, stroke, high blood pressure and various others diseases. If you start using AAS at young age, you may suffer from stunned growth, and TRT a bit later in life is real option, but if you read this blog, you will be aware of that.
One of the better-known side effects of anabolic steroids is roid rage. The condition is defined by extreme moods swings, which may lead to aggressive violent outbursts. Researchers have also observed that users may suffer from paranoid jealousy, extreme irritability, delusions and impaired judgment stemming from feelings of invincibility. Some people just don’t care to know the consequences, they call it the ‘Superman complex’, which is when people view themselves as impervious to a self-destructive behavior pattern. The continued use of steroids is not only due to athletes wanting to enhance their athletic performance, but how they feel about themselves as well. The main reason that people use steroids is image. It’s how certain people value themselves, as maintaining a certain image raises their confidence level and self-esteem
Why Teenagers Should Stay Away From Steroids

Many teenagers do not know exactly how high their natural testosterone production can be. The normal physiologic ranges anywhere from 300 to 1200 ng/dl. This is literally the equivalent of taking a 300mg shot of testosterone (steroids) on a weekly basis. Many times adults get on them through Doctor’s supervision because their natural testosterone production is low. This is what is called Hormone Replacement Therapy (HRT). At a teenager’s age there is not a need to do so as it is very easy to increase size and strength naturally with a good diet and training routine. So many times I hear teens talking about what they want to take or have already done so. What they do not realize is that by using steroids at a young age it will kill your natural testosterone production. This means that when they grow older they will be forced to use them to have a normal testosterone level or they will have a naturally low testosterone. This also means they will not feel as good as they normally would and often not have the stamina that they should have. But let’s face it most young guys that really want to live the bodybuilding lifestyle will start to abuse AAS and GH anyway. They want to be noticed, respect and desired by beautiful willing girls. Young people are already used to take several recreational drugs anyway. Some of us are born with a high natural endogenous level of testosterone. Those guys (and gals) are more prone to risky behavior. Mostly they are more muscular, due to a double or triple amount of testosterone at young age. They are also that are called “blessed with the right genetics” . I guess some of that is true but a higher amount of test also gives them more drive, aggression by training and of course a bigger libido.
Growth Hormone
Human growth hormone (HGH), once an expensive performance-enhancing drug used primarily by elite athletes, has now become cheaply available over the Internet. However, few studies have as yet assessed the prevalence or correlates of illicit HGH use. Anonymous surveys have produced disparate results; an American study claimed that 11 (5%) of 224 10th-grade boys and one (0.5%) of 208 girls had used HGH, but a German survey of 2287 adolescent students found a prevalence of only 0.5% in boys and 0.3% in girls. An anonymous survey of 100 anabolic-androgenic steroid (AAS) users in Wales found that 12 (12%) users reported having tried HGH, and a similar Welsh study nine years later found that the prevalence had risen to 25 (24%) of 102 AAS users. An interview study found only one HGH user (0.6%) among 176 self-declared AAS users (171 men, 5 women) in Wales, and another found only one (4%) HGH user among 25 American women who had used AAS. A subsequent interview study of experienced male weightlifters found that 3 (6%) of 48 AAS users reported lifetime HGH use, and one additional AAS user reported use of the bioactive derivative of HGH, insulin-like growth factor-1 (IGF-I). None of the 45 comparison weightlifters in this study reported use of HGH or IGF-I.
Notably, the above studies were conducted at a time when HGH was more expensive than it is today. By contrast, a recent interview study of 32 AAS users seeking treatment at a Swedish addiction clinic (30 male, 2 female) reported that 15 (47%) had used HGH and 5 (16%) IGF-I. These individuals used many classical drugs of abuse, including cannabis, opioids, and amphetamines – suggesting that AAS and HGH were often part of a larger pattern of poly-substance abuse in this population.
Association between anabolic-androgenic steroid use, anabolic-androgenic steroid dependence, and human growth hormone use in 231 young male weightlifters.
 The 26 men who had specifically taken HGH reported a median (interquartile range) lifetime duration of HGH use of 23 (10, 55) weeks; the 7 men reporting use of IGF-I (6 of whom had also used HGH) reported a median IGF-I use of 9 (8, 10) weeks. Users typically reported using 15–20 units of HGH per week and 50–75 µg/day of IGF-I, but these estimates should be considered approximate, especially given the uncertain authenticity of illicitly obtained preparations. Notably, the 27 HGH/IGF-I users typically reported very long-term AAS use, with a median total lifetime AAS use of 173 (91, 390) weeks. By comparison, the 73 AAS users without HGH/IGF-I use reported a median of only 24 (10, 42) total weeks of AAS use (mean estimated difference in ranks [95% confidence interval] 31.8 [20.8, 42.7]; p < 0.001). Indeed, 22 (81%) of the HGH/IGF-I users had a history of current or past AAS dependence, as diagnosed by modified DSM-IV criteria that we have recently published.28 By contrast only 9 (12%) of the 73 AAS users without HGH/IGF-I use displayed a history of AAS dependence (odds ratio [95% confidence interval]: 28.1 [6.4, 123.2]; p < 0.001).
The 26 men who had specifically taken HGH reported a median (interquartile range) lifetime duration of HGH use of 23 (10, 55) weeks; the 7 men reporting use of IGF-I (6 of whom had also used HGH) reported a median IGF-I use of 9 (8, 10) weeks. Users typically reported using 15–20 units of HGH per week and 50–75 µg/day of IGF-I, but these estimates should be considered approximate, especially given the uncertain authenticity of illicitly obtained preparations. Notably, the 27 HGH/IGF-I users typically reported very long-term AAS use, with a median total lifetime AAS use of 173 (91, 390) weeks. By comparison, the 73 AAS users without HGH/IGF-I use reported a median of only 24 (10, 42) total weeks of AAS use (mean estimated difference in ranks [95% confidence interval] 31.8 [20.8, 42.7]; p < 0.001). Indeed, 22 (81%) of the HGH/IGF-I users had a history of current or past AAS dependence, as diagnosed by modified DSM-IV criteria that we have recently published.28 By contrast only 9 (12%) of the 73 AAS users without HGH/IGF-I use displayed a history of AAS dependence (odds ratio [95% confidence interval]: 28.1 [6.4, 123.2]; p < 0.001).
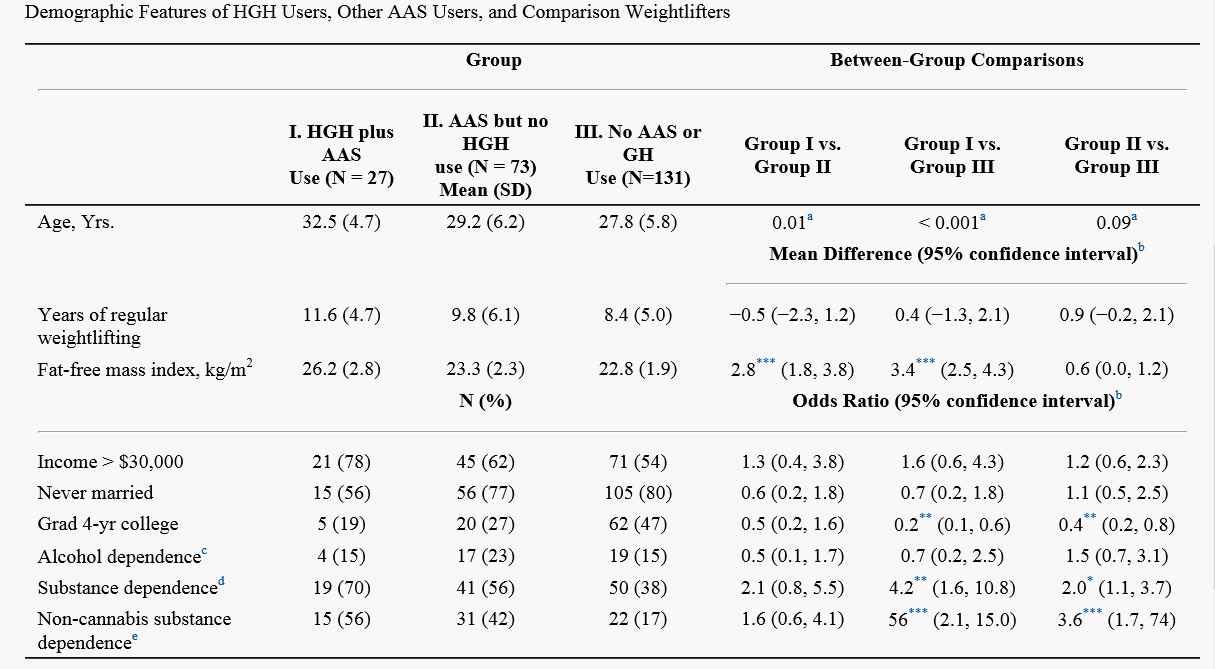
The HGH/IGF-I users were older, had lifted weights for longer, and were strikingly more muscular (i.e., higher in FFMI) than either comparison group (Table 1). The HGH/IGF-I users were the least well educated of the three groups, with only 19% having graduated from college despite their greater mean age. All groups showed a substantial lifetime prevalence of non-alcohol substance dependence, with the HGH/IGF-I users showing the highest prevalence of all. This contrast became even more striking when we deleted cases of cannabis dependence, the most common form of non-alcohol substance dependence. More than half of the 27 HGH/IGF-I users reported a history of dependence on at least one drug other than cannabis or alcohol, including opiates (N = 8), methylenedioxymethamphetamine ("ecstasy") (8), cocaine (7), stimulants (1), and/or polysubstances (1). The prevalence of these forms of substance dependence among the HGH/IGF-I users was slightly higher than among AAS users who had not used HGH/IGF-I, and markedly higher than among weightlifters who had used neither AAS nor HGH/IGF-I.
The 26 men who had specifically taken HGH reported a median (interquartile range) lifetime duration of HGH use of 23 weeks; the 7 men reporting use of IGF-I (6 of whom had also used HGH) reported a median IGF-I use of 9 weeks. Users typically reported using 15–20 units of HGH per week and 50–75 µg/day of IGF-I, but these estimates should be considered approximate, especially given the uncertain authenticity of illicitly obtained preparations. Notably, the 27 HGH/IGF-I users typically reported very long-term AAS use, with a median total lifetime AAS use of 173 (91-390) weeks. By comparison, the 73 AAS users without HGH/IGF-I use reported a median of only 24 (10-42) total weeks of AAS use (mean estimated difference in ranks. Indeed, 22 (81%) of the HGH/IGF-I users had a history of current or past AAS dependence
The HGH/IGF-I users were older, had lifted weights for longer, and were strikingly more muscular (i.e., higher in FFMI) than either comparison group. The HGH/IGF-I users were the least well educated of the three groups, with only 19% having graduated from college despite their greater mean age. All groups showed a substantial lifetime prevalence of non-alcohol substance dependence, with the HGH/IGF-I users showing the highest prevalence of all. This contrast became even more striking when we deleted cases of cannabis dependence, the most common form of non-alcohol substance dependence. More than half of the 27 HGH/IGF-I users reported a history of dependence on at least one drug other than cannabis or alcohol, including opiates (N = 8), methylenedioxymethamphetamine ("ecstasy") (8), cocaine (7), stimulants (1), and/or poly-substances (1). The prevalence of these forms of substance dependence among the HGH/IGF-I users was slightly higher than among AAS users who had not used HGH/IGF-I, and markedly higher than among weightlifters who had used neither AAS nor HGH/IGF-I.
In an ongoing study of 231 experienced male weightlifters aged 18–40, we found that illicit HGH use is common, often prolonged, and closely associated with abuse of or dependence upon both AAS and classical drugs – a finding consistent with the European data cited earlier. In this context, it is difficult to determine whether HGH abuse arises solely as a comorbid substance abuse disorder in a population with high rates of AAS use and of classical substance dependence, or whether prolonged HGH use might develop into a true chemical dependency in its own right. Although HGH does not produce a “reward” of acute intoxication in the manner of classical dependence-inducing drugs such as alcohol or opioids, the possibility remains that its metabolic effects, or perhaps even subtle hedonic effects, might themselves be sufficiently reinforcing to induce a dependence syndrome in some individuals. Further studies of the neurobiology underlying HGH abuse will be needed to understand this distinction more fully.
 Notably, the 27% prevalence of lifetime HGH/IGF-I use among AAS users in the present study was significantly greater than the 8% prevalence among 48 AAS users in our similar previous study of weightlifters. Likely reflecting the increasing availability and decreasing price of HGH in recent years. When interpreting these findings however, it should be recognized that young male weightlifters, while probably the largest consumers of HGH, are not the only population that uses this hormone illicitly. In particular, many non-weightlifters, often older than age 40, receive prescriptions for HGH from “anti-aging” clinics, compounding pharmacies, and other possibly illegal sources.These individuals likely differ from the population evaluated in the present study.
Notably, the 27% prevalence of lifetime HGH/IGF-I use among AAS users in the present study was significantly greater than the 8% prevalence among 48 AAS users in our similar previous study of weightlifters. Likely reflecting the increasing availability and decreasing price of HGH in recent years. When interpreting these findings however, it should be recognized that young male weightlifters, while probably the largest consumers of HGH, are not the only population that uses this hormone illicitly. In particular, many non-weightlifters, often older than age 40, receive prescriptions for HGH from “anti-aging” clinics, compounding pharmacies, and other possibly illegal sources.These individuals likely differ from the population evaluated in the present study.
- Login to post comments