
Narcotic and Non-narcotic Painkillers

A painkiller (also called pain killers, pain medications, pain relievers) and medically known as an analgesic is defined as a drug used to relieve pain, or achieve analgesia, by blocking pain signals going to the brain or by interfering with the brain's interpretation of the signals. There are basically two kinds painkillers or analgesics: non-narcotic and narcotic.
Most of you reading this blog-post know that professional and high level bodybuilders (and wrestlers, powerlifters etc) used and use. But exactly how dangerous are these painkillers and do they interfere with muscle hypertrophy (muscle growth)?
In a blogpost in 2014 I wrote about the prescription drugs and recreational drugs that is common in high-end bodybuilding. But does breaking piankillers in narcotic and non-narcotic painkillers, like NAISD’s ,mean that the latter is innocent for the bodybuilder in terms of health and muscle growth?
What we know is risky.. is the polypharmacy and the narcotic painkillers.
C raig Titus: “Crystal Meth for dieting to suppress appetite, cocaine to suppress appetite, and dry skin out for stage, pain relievers to eliminate joint pain, Zanax, Valum, Ambien to sleep, it’s all being used on a regular basis.”
raig Titus: “Crystal Meth for dieting to suppress appetite, cocaine to suppress appetite, and dry skin out for stage, pain relievers to eliminate joint pain, Zanax, Valum, Ambien to sleep, it’s all being used on a regular basis.”
“Nubain, or Naluphine is a very effective aid while preparing for contest during severe dieting as well as an excellent pain reliever during and fallowing training sessions.” A few quotes from the forums:
“This is a bit extreme. Painkillers dull the pain don't eliminate it in any sense. Training on Nubain is great because you can push harder and longer. You still get to the point of muscle failure but not as fast. It's not like you can take a narcotic and train through a muscle tear or something. That being said using narcotics is a poor choice because controlling how and when you use them is almost impossible.”
“But, training on a pain killer will definitely give you a better workout. And when you're pre contest and on a bunch of anabolic steroids you are able to over train and get benefits from it. Also, pre contest prep is brutal. It fucks with you in many ways, the worst being the inability to relax and sleep. If from a low carb diet, a brutal work-out or drugs like Clenbuterol and Ephedrine (or ECA) sleeping patterns become crazy and some just can't sleep at all. A narcotic like Nubain eliminates these problems and makes prep almost easy. It's not a good idea but neither is 90% of the other things that competitive bodybuilders do. I was probably less healthy 15 years ago when I was competing than now. No doubt about it something like Nubain is helpful to the competitive bodybuilder. Does that make it a smart thing to do, hell no.”
“Using narcotics or anti-anxiety drugs to get high has no place in competitive bodybuilder. But these drugs can be helpful if used correctly. Amphetamines are great when carbs are low a few weeks out, plus they cut your appetite. Am I saying to do this? Not at all but it is what bodybuilding is. Anything and everything is used to get an edge.”
Narcotics are also called opioid pain relievers. They are used only for pain that is severe and is not helped by other, milder types of painkillers. Forty-five people die every day from opioid (narcotic) prescription painkiller overdoses – more deaths than heroin and cocaine.
According to recent figures from the US Drug Enforcement Administration (DEA), in the last ten years the number of painkillers sold and distributed in the United States has risen by 600%. Most of the increased sales are painkiller pills that contain oxycodone, the active ingredient in the painkiller OxyContin, once known as "hillbilly heroin".
Taking anti-inflammatories may help nagging injuries in the short run, but their long-term use is questionable.
W ith big muscles come big-time aches and pains. Like anything in this world, bodybuilding will place strain on your body over time. If you don’t take the proper precautions, you’ll end up with big muscles attached to joints that ache all day long. You’ll have a spine that can’t support a load. You’ll have shoulders that grind and crunch. And if you’re not careful, you’ll end up with a pain killer addiction like many professional athletes. You want to prevent all this beforehand.
ith big muscles come big-time aches and pains. Like anything in this world, bodybuilding will place strain on your body over time. If you don’t take the proper precautions, you’ll end up with big muscles attached to joints that ache all day long. You’ll have a spine that can’t support a load. You’ll have shoulders that grind and crunch. And if you’re not careful, you’ll end up with a pain killer addiction like many professional athletes. You want to prevent all this beforehand.
If you’ve been weight training for any appreciable length of time, chances are you’ve encountered an overuse injury such as tendonitis or bursitis at some time in your career. Because of the repetitive nature of weight training, overuse injuries are for all intents and purposes part of the game. Although careful attention to detail in your exercise program (i.e. allowing enough recovery time between workouts, proper manipulation of sets/reps/weight, etc.) can help to minimize these injuries, they still occur.
Recovering from overuse injuries typically requires some form of rest from activities that aggravate the injury. Unfortunately, many serious bodybuilders often view rest as a form of weakness. Rather than taking time off for injuries to heal, some people search for other methods to help them get through their workouts.
One common quick fix is to use an over-the-counter nonsteroidal anti-inflammatory drug (NSAID) such as ibuprofen (e.g., Motrin, Advil) or sodium naproxide (Aleve). Desperate bodybuilders often seek out prescription-grade NSAIDs, that are higher in dosage than their over-the-counter counterparts or reach for narcotic painkillers.
Does an NSAID a day keep satellite cells at bay?
M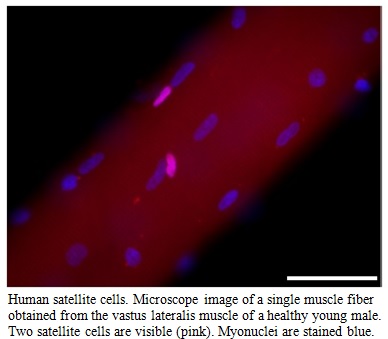 ackey 2013: Nonsteroidal anti-inflammatory drugs (NSAIDs) are widely consumed by athletes worldwide, despite growing evidence for a negative influence on the adaptation of skeletal muscle to exercise, at least in young healthy individuals. This review focuses on the potential of NSAIDs to alter the activity of satellite cells, the muscle stem cell responsible for repair and maintenance of skeletal muscle. The signaling pathways that are potentially modified by NSAID exposure are also considered. Growth factors as well as inflammatory cells and connective tissue appear to be key factors in the response of muscle under conditions where cyclooxygenase and prostaglandin activity are blocked through NSAID ingestion or infusion. Discrepancies in the literature regarding the response of young and old individuals are addressed, where it appears that the elderly may benefit from NSAID ingestion,
ackey 2013: Nonsteroidal anti-inflammatory drugs (NSAIDs) are widely consumed by athletes worldwide, despite growing evidence for a negative influence on the adaptation of skeletal muscle to exercise, at least in young healthy individuals. This review focuses on the potential of NSAIDs to alter the activity of satellite cells, the muscle stem cell responsible for repair and maintenance of skeletal muscle. The signaling pathways that are potentially modified by NSAID exposure are also considered. Growth factors as well as inflammatory cells and connective tissue appear to be key factors in the response of muscle under conditions where cyclooxygenase and prostaglandin activity are blocked through NSAID ingestion or infusion. Discrepancies in the literature regarding the response of young and old individuals are addressed, where it appears that the elderly may benefit from NSAID ingestion, 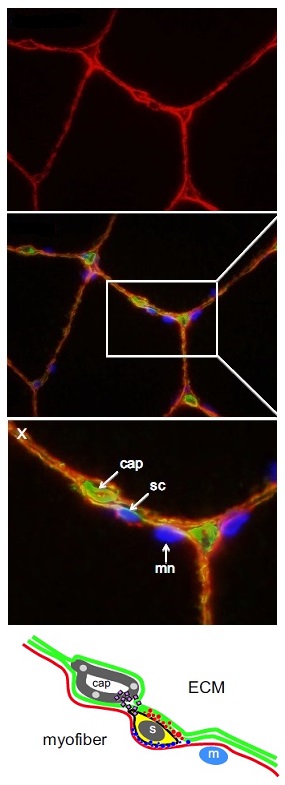 although this clearly requires further study. The long-term implications for the muscle of the apparent inhibitory effect of NSAIDs on satellite cells in younger individuals are not clear, and it is possible these may first become apparent with chronic use in athletes training at a high level or with advancing age. Reports of the potential for NSAIDs to alter prostaglandin and growth factor signaling provide a basis for further study of the mechanism of NSAID action on satellite cells.
although this clearly requires further study. The long-term implications for the muscle of the apparent inhibitory effect of NSAIDs on satellite cells in younger individuals are not clear, and it is possible these may first become apparent with chronic use in athletes training at a high level or with advancing age. Reports of the potential for NSAIDs to alter prostaglandin and growth factor signaling provide a basis for further study of the mechanism of NSAID action on satellite cells.
On the left: satellite cell environment. Microscope image of a cross section of a vastus lateralis sample obtained from a young healthy individual.
Image X is a higher magnification of the indicated region of the merged image. One satellite cell (sc) is visible, situated between the myofiber plasmalemma (red) and the basement membrane (green). Note the different location of the myonucleus (mn), situated inside the myofiber plasmalemma. A capillary (cap) is visible in green in close proximity to the satellite cell. Nuclei are stained blue.
Schematic based on X, illustrating the location of different receptors (red and blue circles) on the extracellular matrix (ECM, green lines) and myofiber (red line) sides of the satellite cell (s) envelope. It is believed that these receptors exert different signaling to direct the fate of the new satellite cells to either fuse with the fiber or to remain as a satellite cell to maintain the satellite cell pool. This schematic also depicts the bidirectional release of growth factors that has been demonstrated to exist between satellite cells and endothelial cells making up the capillaries (cap). A myonucleus (m) is also shown, situated under the sarcolemma (red line).
“No pain, no gain” may keep you motivated during an intense workout, but what happens when you can’t move the next day? If aspirin or Advil are on your mind, first take a look at what these pain meds may be doing to your muscle growth.
First off, pain meds aren’t all bad. Sore muscles after a workout come with the territory, especially if you’re tackling new types of exercises. Dulling the pain a little can help you get back to the gym and push through your next workout.
Long-term use of some pain relievers, though, can damage your liver and lead to headaches and they might also be stunting your muscle growth.
From the research of Mackey 2013 as printed above about the downsides of NSAIDS (non-steroid pain meds like aspirin and ibuprofen) on muscle growth, what you need to know:
For recreational athletes: Occasional use of NSAIDs according to package instructions is not likely to have any negative effects on muscle development and regular use shouldn't affect muscle growth over the short term.
For elite athletes or those looking to maximize your muscle growth: Long-term use of NSAIDs could keep you from hitting your muscle targets.
More Bad News About NSAIDs Reported (2013)
W hile no analgesic therapy is risk-free, adverse cardiovascular and gastrointestinal events associated with nonsteroidal anti-inflammatory drugs (NSAIDs), including the newer generation selective-COX-2 inhibitor (COXIB) NSAIDs, need to be fully appreciated for the sake of the users safety. A newly reported, and largest of its kind, meta-analysis of randomized, controlled trials (RCTs) provides further confirmation that these analgesic agents pose noteworthy risks of heart problems, stomach disorders, and death — all of which call for their more cautious use in patients with chronic pain conditions.
hile no analgesic therapy is risk-free, adverse cardiovascular and gastrointestinal events associated with nonsteroidal anti-inflammatory drugs (NSAIDs), including the newer generation selective-COX-2 inhibitor (COXIB) NSAIDs, need to be fully appreciated for the sake of the users safety. A newly reported, and largest of its kind, meta-analysis of randomized, controlled trials (RCTs) provides further confirmation that these analgesic agents pose noteworthy risks of heart problems, stomach disorders, and death — all of which call for their more cautious use in patients with chronic pain conditions.
T he coxibs examined included celecoxib, rofecoxib, etoricoxib, and lumiracoxib, while the traditional NSAIDs studied were primarily diclofenac, ibuprofen, and naproxen.
he coxibs examined included celecoxib, rofecoxib, etoricoxib, and lumiracoxib, while the traditional NSAIDs studied were primarily diclofenac, ibuprofen, and naproxen.
In trials providing individual participant baseline data, mean age was 61 years, roughly two-thirds were female, and 79% were white. And most trials of traditional NSAIDs involved high-dose daily regimens — diclofenac 150 mg/d, ibuprofen 2400 mg/d, naproxen 1000 mg/d.
The main outcomes of concern in the meta-analysis were major vascular events — including nonfatal MI, nonfatal stroke, or vascular death — as well as major coronary events (nonfatal myocardial infarction or coronary death), stroke, heart failure, and upper gastrointestinal complications (perforation, obstruction, or bleed). Key findings of the study, published online in The Lancet, included the following:
Coxib therapy significantly increased occurrences of major vascular events by about one-third, as did diclofenac. These effects were chiefly due to increases in major coronary events. Ibuprofen also significantly increased major coronary events, but not major vascular events. Naproxen did not significantly increase major vascular or coronary events.
Vascular-related deaths were increased significantly by coxibs and diclofenac, but not by ibuprofen or by naproxen.
The Rate Ratios for heart failure requiring hospitalization were roughly doubled by all NSAIDs, and all NSAID regimens significantly increased upper GI complications: coxibs RR=1.81; diclofenac RR=1.89; ibuprofen RR=3.97and naproxen RR. There was no evidence of increased stroke risk with any of the NSAIDs studied.
In balance, This are shocking figures, but how seriously should we take them? A meta analyses on sick people (mean age was 61 years) on longtime, high dose of NSAIDs. While the outcomes were statistically significant and clinically serious, the incidence rates and absolute excess risks were of small size. For example, compared with placebo, therapy with a coxib or high-dose diclofenac for 1 year was associated with about 3 additional major vascular events per 1000 person-years (0.3% incidence rate), with 1 such event causing death (0.1% incidence rate), as said in sick old people that used high doses, how could we extrapolate those numbers (even when used on the net frequently with regards on dangers of using NSAIDs), to healthy young bodybuilders? ..NOT..
