
Interleukins (cytokines)

In August 1995 Quinn et al released a study called “Interleukin-15: a novel cytokine anabolic for skeletal muscle.”
We all know most pro-bodybuilders don’t read all the new studies, but most athletes hire people that make a living by supervising professional bodybuilders and other athletes such a tennisplayers, footballplayers, cyclists etc etc.. In bodybuilding were nutrition and supplementation is very important these people are mostly called “nutritionists.”
As Dr Larkins from Australia said: "There's a whole generation of sports science people coming through who are well trained in sports performance areas and what I call genuine  areas but many, many sports and clubs have got these people.”
areas but many, many sports and clubs have got these people.”
Well the keywords “anabolic for skeletal muscle” did ring a bell. Of course bodybuilders already worked with other interleukins, like by example IL-6. Soon several studies on Il-15 popped up, also again from Quinn in 2002 “Overexpression of interleukin-15 Induces skeletal muscle hypertrophy in vitro.” Most studies were performed on rodents in high amounts. Thus it was hard to translate results to bodybuilders and athletes dieting and training hard.
Quinn in 1995 discovered that Il-15 was superior to IGF-1, but that it also worked synergistically with IGF-1. In vitro (test tube) MHC (myosin heavy chain) accumulation with the addition of this ‘novel cytokine’ individually and with IGF-1 synergism. “IL-15 used at 10 ng/ml doubled MHC accumulation and was as effective as IGF-I used at 10 or 100 ng/ml. IL-15 and IGF-I used together increased MHC accumulation close to five-fold, indicating these two factors can act additively on muscle fibers.”
At the beginning of the 2000’s rumours went that Markus Rühl used IL-15. Brock Strasser from T- Magazine, who previously reported on the use of IL-15 by bodybuilders, wrote that IFBB-pro-bodybuilders also used Epidural Growth Factor. Strasser: “These means are emerging as noveau drugs for the bodybuilding elite."Brian Batcheldor wrote in T-magazine that he was doing experiments with IL-15 and Leukemia Inhibitory Factor (LIF). From LIF we already know that it accelerates the recovery of injuries. Used together with IL-15, LIF increases the amount of myosin in the muscle fibers by 500 percent. Batcheldor: "Unfortunately, the limiting factor thesis with growth factors is price - you will probably never be able to afford the optimal dosage.”
But, that wasn’t all. Later on research in vivo was performed using rats and administration of IL-15. The results showed a 33% decrease in white adipose tissue, and while it did augment protein synthesis and degradation, it failed to cause a hulk-rat....
 Luckily, that research did lead into studying a very interesting aspect of IL-15, which is it’s genetic component. Again, using genetically different rats (either leptin-receptor negative or leptin deficient), and again, the results in the control and leptin deficient rats showed a reduction in white adipose tissue without changes to food intake, awesome! Unfortunately, the results in the leptin-receptor negative was so great, with practically no action. However, what was shown was an 84% reduction in the gamma receptor signaling subunit, meaning, that for that type of genetic difference, IL-15 would not have the direct action on white adipose tissue as the normal population. From that research, the role of IL-15 was becoming more clear, in terms of myoblast differentiation, protein metabolism augmentation, adipose tissue signaling and how it works, but just nothing in humans,yet.
Luckily, that research did lead into studying a very interesting aspect of IL-15, which is it’s genetic component. Again, using genetically different rats (either leptin-receptor negative or leptin deficient), and again, the results in the control and leptin deficient rats showed a reduction in white adipose tissue without changes to food intake, awesome! Unfortunately, the results in the leptin-receptor negative was so great, with practically no action. However, what was shown was an 84% reduction in the gamma receptor signaling subunit, meaning, that for that type of genetic difference, IL-15 would not have the direct action on white adipose tissue as the normal population. From that research, the role of IL-15 was becoming more clear, in terms of myoblast differentiation, protein metabolism augmentation, adipose tissue signaling and how it works, but just nothing in humans,yet.
In 2003 one of the first ‘human’ papers was introduced on IL-15 in comparison to actions of IGF-1 on myogenic cells. The results were definitely interesting, in that they showed that the actions were completely different in humans. While IGF-1 was acting ‘precursory’ myoblasts, IL-15 was carrying out the action of hypertrophy by causing myosin heavy chain accretion AFTER differentiation occurred. In summary, it was showing another piece of the puzzle that was previously unknown, and not just for bodybuilders, but for muscle wasting patients.
“Taken together, these observations suggest that additional research into the action of IL-15 may be beneficial for developing treatment options for muscle wasting”
As interesting as all this mechanism of action stuff is, I’m sure the important thing to most people reading this is, “What does it mean to me?” Well, there are some incredibly interesting studies showing how that ‘genetic factor’ of IL-15 can come into play. One of the most fascinating was published in 2004 and looked at different IL-15 receptor genetic variations and how that impacted on resistance training adaptations.
They used 153 people with almost no resistance training experience and put them on a 10 week 3x per week resistance exercise training (RET) program that used progressive overload in a 6-10 rep range while testing for 1RM as well, and it showed pretty fascinating result.
Of those that had the AA variant of the receptor gene, they exhibited the highest hypertrophy increase, while also presenting the lowest increase in strength. Contrast with those who had the CC variant, who had the lowest hypertrophy increase yet the highest strength increase, and then there were those ‘middle of the ground CA’s who were .... middle of the ground in terms of specific responsiveness. Now, above all the other intra-muscular actions, we finally had a reason to call ourselves special snowflakes. Unfortunately, those types of things (genetic variants) can’t really be controlled.
So, what can you do if you want to try to increasing your IL-15 levels?
For one, calorie restriction has been shown to work, newer research has shown that, in animals (dang rats again) that CR can preserve to a point, the declination in IL-15 that is usually accompanying senescence, and possibly help with sarcopenia and age related weight gain. Plus, even walking and light exercise has been shown to increase those levels, and I would bet that those IL-15 secretions would be in assistance to weight loss as well.
So, there we go, a myokine that does everything from weight loss, to muscle gain, activating mTOR to attenuating sarcopenia, to helping with obesity, and maybe even showing us what that ‘overtraining syndrome’ is caused by. (Hint: there are IL-15 receptors that impact CNS function as well)
 It’s no secret that resistance training leads to an increase in muscle mass, referred to as muscle hypertrophy. While scientists may agree on this, there is still much debate on how this very complex process takes place. To many, muscle growth occurs from simply lifting weights, eating ample nutrients, and resisting the trained muscle. The sequence of events that must occur in order for muscle tissue to grow appears to be much more complex than this.
It’s no secret that resistance training leads to an increase in muscle mass, referred to as muscle hypertrophy. While scientists may agree on this, there is still much debate on how this very complex process takes place. To many, muscle growth occurs from simply lifting weights, eating ample nutrients, and resisting the trained muscle. The sequence of events that must occur in order for muscle tissue to grow appears to be much more complex than this.
Muscle hypertrophy is an increase in muscle mass due to an increase in size of individual muscle fibers. Skeletal muscle adapts to regular, increasing workloads that exceed what was once the capacity of the muscle fiber, and the muscle becomes more efficient at transmitting forces. By applying progressive levels of stress to skeletal muscle, it must also adapt by increasing the size and amount of contractile proteins within each muscle fiber, leading to an increase in the size of the muscle itself. This process may seem rather simple, but a closer look will prove the process to be much more complicated.
Resistance exercise causes trauma to skeletal muscle. The immune system then responds with a sequence of reactions that lead to inflammation in the area where the damage occurred. The purpose of the inflammation is to contain the damage, repair the damage, and clear the area of waste products. When muscles are damaged, cytokines are produced at the site of the damaged cells. Cytokines are proteins, which serve as directors of the immune system. They are responsible for the arrival of lymphocytes, neutrophils, monocytes, and other healer cells to the damaged area. The cytokines that produce most of the inflammatory response are Interleukin-1 (IL-1), Interleukin-6 (IL-6), and tumor necrosis factor (TNF.) These cytokines are responsible for protein breakdown, removal of damaged cells, and an increased production of hormone-like substances that help control the inflammation called prostaglandins. The immune system plays an important role in muscle repair and growth.
Overstraining syndrome often occurs when the immune system is not able to handle the amount of muscle tissue that is damaged, and this leaves a person vulnerable to injury and illness over time.
Satellite cells function to facilitate growth, maintenance, and repair damaged muscle tissue. Satellite cells are located on the outer surface of the muscle fiber. These cells are dormant, but become activated when the muscle receives any sort of damage, such as what occurs during resistance training. The activated satellite cells multiply and are drawn to the site where damage occurred. For example, if shoulders were trained, that is where these satellite cells would end up. After they reach the site, they fuse to the muscle fiber, donating their nuclei to help regenerate the muscle fiber. This process increases the size of the muscle fibers and the number of contractile proteins, (myosin and actin,) within the fiber. This satellite cell activation period lasts up to 48 hours after the muscle is damaged from training. This period solidifies the importance of rest for muscle growth to take place.
Hormones are chemicals which organs secrete in order to regulate the activity of an organ or group of cells in the body. Hormone function is affected by nutritional intake, lifestyle, and general health. There are several hormones that play an important role in muscle hypertrophy.
 Growth hormone is a peptide hormone that stimulates insulin growth factor (IGF) in skeletal muscle, which promotes satellite cell activation. This results in an increase in contractile proteins present in the muscle fibers, and an increase in the size of the muscle fibers.
Growth hormone is a peptide hormone that stimulates insulin growth factor (IGF) in skeletal muscle, which promotes satellite cell activation. This results in an increase in contractile proteins present in the muscle fibers, and an increase in the size of the muscle fibers.
Growth factors are highly specific proteins that are very involved in muscle hypertrophy. Without their involvement, muscle growth is not likely to occur.
Insulin, like growth factor (IGF) is secreted by muscle tissue. It regulates insulin metabolism and stimulates protein synthesis, which are both vital to hypertrophy. In response to resistance exercise, endogenous levels of IGF are substantially elevated. The importance of IGF for muscle growth has led to exogenous IGF to become very popular among bodybuilders.
Hepatocyte growth factor, (HGF,) is a cytokine that activates satellite cells and is responsible for causing satellite cells to travel to the injured muscle tissue for repair.
Fibroblast growth factor, (FGF) is stored in skeletal muscle in nine different forms. Five of these forms initiate satellite cells to multiply, so they can aid in skeletal muscle repair and growth. The amount of FGF released is proportional to the degree of muscle damage.
Muscle growth is a multidimensional process, with many factors involved. It involves a complex interaction between satellite cells, the immune system, hormones, and growth factors to facilitate muscle growth. A deficiency in any one of these areas can slow muscle growth and ultimately lead to catabolism (muscle breakdown.) While an in depth knowledge of the processes of muscle hypertrophy is not required to experience muscle growth, a basic understanding on how the body repairs itself after resistance training is important for anyone wanting to maximize their muscle growth potential.
Bodybuilders by themselves or with help of a trainer now inject many of those substances into their body, substances such as AAS, rhGH, IGF-LR3, MGF, insulin, all kinds of other peptides, SARMs and also interleukins. Leading to monstrous bodybuilders.
Use and dosage
What is known on its use and dosing? From the 1995 study that draw the attention of bodybuilders they knew, that the combined administration (stacking) of interleukin-15 and IGF-1 resulted in an synergistical effect that included a 500% increase in muscle-specific heavy chain myosin (muscle growth). So rumors are some of the pro’s are using this stack others claim a combination of IL-15 and MGF. But as with all new innovative compounds the exact use is kept secret.
In the past bodybuilders used veterinary versions of insulin and growth hormone, porcine slin was mostly used without a problem since it is almost similar to the human version and the modified version was even better. Buying a small amount of very pure recombinant human Interleukin 15 is very expensive varying from 3500 – 2700 USD/gram
It’s easy to do a math how much a dose of 50-80 mcg/day would cost. Or as we did in the early days of rhGH use, take a few days off (5 on 2 off). Or use only after you trained and in the muscle-group you trained.
Cutting it with other growth factors will not only work synergistically but will also provide a workable/effective doses. It is said guys do site-injection.I think it can take a while before members keep a log on the forums. But I’m very interested in future developments with this compound
Genetic switching mechanism behind muscle growth unraveled
If you train your muscles they grow. But how does this work exactly? Natural bodybuilders are the walking proof that muscles grow when you train a lot. It is a known phenomenon: if your muscles are used regularly, they are going to grow. Bodybuilders are the walking proof. But actually the growth of muscles is quite an extraordinary phenomenon. Why would something you frequently use does not wear out, but rather becomes stronger? And how does your body know your muscles must be convalesced? A group of French cell biologists (Guerci et all 2012) has solved a new piece of the puzzle of muscle growth. They did a series of experiments on both live mice 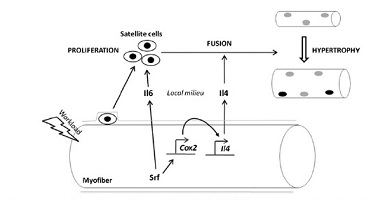 as pieces of mouse muscle they grew in their lab.
as pieces of mouse muscle they grew in their lab.
Schematic model left: in response to increased workload, Srf within myofibers (musclefibers) modulates Il-6 and Cox2/ Il-4 expressions and, therefore, exerts a paracrine control of satellite cell proliferation and fusion respectively, which in turn supports skeletal muscle hypertrophy (muscle growth).
First a little explanation about what muscles exactly are. At the most basic level they consist of elongated muscle cells chock full of protein. The key proteins in muscle cells are actin and myosin. These proteins both form long chains. During the contraction of your muscles, these protein chains are moving past each other, causing all the muscle cells to become a bit shorter.
It was already known that muscles can be strengthened in two ways: by creating additional muscle cells, or by creating additional protein chains into existing muscle cells so they can contract better. Aline Guerci and her colleagues were particularly interested in the first mechanism, the production of extra muscle cells. They already knew that muscle after training create certain substances called interleukins. And also that these interleukins (for those who want to know more precisely, interleukin-4 and interleukin-6) in the body present muscle precursor cells encourage to grow into mature muscle cells and to attach themselves to existing muscle cells.
But how do the muscle cells know they need to create interleukins after intensive training? Cells never produce just any substances that they, in theory, can create. The genes encoding for the substances may be on or off, and may be more or less active. The main indication for Guerci and her team what the genetic control mechanism behind the production of interleukins by muscle cells could be, was that in both humans and mice, the amount of serum response factor (SRF) in the muscles deteriorate as they grow older. And the older you are, the less able to grow your muscles. Could this Srf might be the substance which regulates the activity of the interleukin-genes?One of the best ways you can check this is by culturing organisms that have no Srf by a mutation in their DNA. In this case, Guerci bred Srf-less mice. And indeed, how heavy the muscles of these mice were also charged, they made no interleukins and were not growing. After all kinds of additional tests, the French were sure: Srf is the first link in the chain that led muscles to grow impetus after exercise. It picks up the movement of the muscle cell, and put the underlying genetic mechanism towards muscle growth into operation.
Now, all this is known, it gives hope to all people who suffer from weakened muscle by, for example, a disease or a long period of enforced bed rest. Possibly they may be helped by, for example, administer extra Srf, or any of the interleukins which are created by this rule substance. But whether this actually works this way should (and will) be investigated further.