
Influences on the halflife and potency of steroids

 I want to catagorise some known and unknown influencing factors on the half-life and potency of injected steroids.
I want to catagorise some known and unknown influencing factors on the half-life and potency of injected steroids.
Many factors determen the effect of a active componenet solved in an oily depot. That is the oily carrier itself, the preservative that is used to protect the oily injectable against bacteria and fungus. Then sometimes a solvent and a co-solvent is used, these solvents are also responsible for the viscosity and syringability. Meaning? The viscosity (thickness) of the oily injectable comes from the oily carrier, the solvent mostly benzyl benzoate and some co-solvents such as Ethanol, isopropyl alcohol, gauiacol and co-solvents such as Ethyl Oleate.
.jpg) Syringability means that the injectable should be easy to inject, this is partly due to the API (raw powder) that should be Ultra Fine, older athletes remember the Winstrol-V that needed a big needle to inject, modern human grade powders are very fine because they have been milled through a nano-mill. This the contrary to vetrinairy powders or some UG labs that buy cheaper powder (mostly also not as pure as they should be).
Syringability means that the injectable should be easy to inject, this is partly due to the API (raw powder) that should be Ultra Fine, older athletes remember the Winstrol-V that needed a big needle to inject, modern human grade powders are very fine because they have been milled through a nano-mill. This the contrary to vetrinairy powders or some UG labs that buy cheaper powder (mostly also not as pure as they should be).
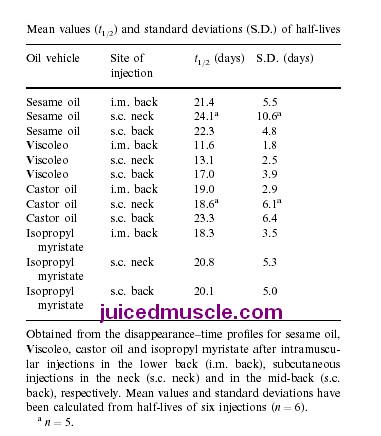
As you can see in the table on the right the veggie oils contain many different fatty acids and every different batch has different amounts of these fatty acids. A synthetic oil like Ethyl oleate is compared to that stable and contains only one fatty acid. An other very good synthetic oil is Migyol 812.
The table on the right also shows the viscosity, which on its turn influences tha dissappearance rate from the injectionspot. Some consequent studies in Sweden by Susan Wang done on pigs (very simular to humans for this reason) also showed that that viscosity and dissapearence rates are corrolated. Pay special attention to castor oil in both tables since this specific oil was used in other spectacular study that made clear to all bodybuilders and bodybuilder discussionforums that all those so carefull made list on halflifes of estrified steroids where useless.
 In the search for long-acting testosterone preparations suited for substitution therapy of hypogonadal men (Behre et all, 1999), testosterone undecanoate (TU) dissolved in either tea seed oil or castor oil was investigated.
In the search for long-acting testosterone preparations suited for substitution therapy of hypogonadal men (Behre et all, 1999), testosterone undecanoate (TU) dissolved in either tea seed oil or castor oil was investigated.
* In study I, 1000 mg TU in tea seed oil (125 mg/ml) were injected in equal parts into the gluteal muscles of seven hypogonadal men.
* In study II, 1000mg TU in castor oil (250 mg/ml) were injected into one gluteal muscle of 14 patients.
Results:
In comparison with published data on testosterone enanthate, most widely used for i.m. injections, the kinetic profiles of both TU preparations showed extended half-lives and serum levels not exceeding the upper limit of normal.
The TU-castor oil preparation had a longer half-life than TU in tea seed oil 34 vs 21 days
Intramuscularly injected TE (Testosterone Enanthate) is the most widely used testosterone preparation when depot effects are required, e.g. for substitution of hypogonadism orin trials for hormonal male contraception . However,after injection of the commonly administered dose of 200 or 250 mg, TE has the disadvantage that it produces supraphysiological serum testosterone levels during the days immediately following administration with a slow decline to the lower limit of normal following within 10–14 days (11). Patients dislike these swings in serum testosterone levels, which they experience as ups and downs in vigour, mood and sexual activity. Other testosterone esters in clinical use such as testosterone cypionate or cyclohexanecarboxylate show pharmacokinetic profiles almost identical to that of TE , so that these preparations offer no therapeutic advantage. Although the current study deals with a much higher dose of testosterone than administered in previous studies, TU does not result in supranormal serum testosterone levels, but in much prolonged action. Extrapolating from single-dose kinetics it appears that upon repeated injections of 1000 mg, injection intervals of 6–10 weeks will be possible. The prolonged intervals and the normal serum testosterone levels throughout the injection-free period would be welcomed by the hypogonadal patient requiring substitution as well as by the eugonadal male seeking contraceptive protection. Although different routes of administration may yield different toxicological profiles for the same drug, the lack of serious side-effects from TU administered orally at doses of 80–160 mg/day over many years gives reason to assume that TU applied intramuscular would be safe too.
An older but eye opening research ON HUMANS (Minto et all, 1996) showed new results.
Volume and Concentration
Steroids come in all shapes and sizes. In other words, you can find nandrolone (or Testosterone or boldenone) esters in 25 mg/ml, 50 mg/ml, 100 mg/ml, 200 mg/ml and so forth. Is a 400 mg injection using two milliliters of a 200 mg/ml oily solution the same as using four milliliters of a 100 mg/ml solution? After all, the net amount is still 400 mg, right? Unfortunately, this isn?t the case.
Steroid concentration in the solution greatly affects the dynamics and kinetics. In this study, some of the men received a 100 mg/ml injection of nandrolone decanoate and other men received a 100 mg injection using a 25 mg/ml solution (which means they received four milliliters, of course). Those that received the 100 mg/ml injection reached significantly higher (between 30% and 50%) plasma levels of nandrolone than those who got 100 mg via the 25 mg/ml solution. To top it off, the 100 mg/ml group?s plasma nandrolone level stayed elevated for a little bit longer; however, the length of suppression of endogenous Testosterone was almost identical.
What does this tell us? It tells us that if we want to maximize plasma levels of hormone (and thereby, maximize gains in lean muscle) we want to opt for the most concentrated version of whatever steroid(s) we decide we're going to use. If we're using Testosterone, we surely want to use a 200mg/ml enanthate over something like 100mg enanthate. If we're using nandrolone, we want to use 300mg/ml stuff over 50mg/ml or 100mg/ml nandrolone decanoate made by others.
Injections Sites
Another thing that superficially seems trivial but makes a huge difference in plasma steroid concentrations is where you inject. That?s right, this seems utterly trivial but this study concluded that gluteal injections yielded far superior plasma levels as opposed to injections in the deltoid.
Of all the locations that nandrolone injections were given in this study (100 mg/ml x 1 ml in the glutes, 25 mg/ml x 4 ml in the glutes and 100 mg/ml x 1 ml in the deltoid), the deltoid injections yielded the lowest plasma levels of nandrolone by a huge factor, with peak concentrations being 50% lower than the 100 mg/ml gluteal injection and around 10% lower than the 100 mg/ml x 4ml gluteal injection. Lesson learned here: Only inject in the glutes for maximal steroidal efficacy.
Potency
A study (Weinbauer et all, 2003) on monkeys studying the potency of Testosterone Enanthate – Undecylenate and Buciclate, showed that 100 mg Testosteron Undecanoate (100 mg pure testosterone base, thus without the esterweight) was (at least) 2,5times as effective as 100 mg Testosterone Enanthate. Which means that this study proved that the estrification has a definite influence on the bioavailability and that longer (slower) estrifications give more potency to the parentcompound.
Optimal dosage
We use AAS to achieve a certain effect for athletic or cosmetic reasons. This usage provides the wanted effects (muscle mass) and unwanted effects (side-effects like gynaecomastia [ bitch tits]. To find the optimal balance, some studies try to find the best dose that still provides the wanted effects with the less possible side-effects. Off course hard-core bodybuilders don’t actually care, because they add anti-estrogens to their stack and many other drugs to fight the side-effects. Still i.m.o. interesting to post for the older and the cautious athhltes that want to add a small bit of chemical aid to benefit their hard training and overall wellbeing
(Bhasin et all 2005) Older men are as responsive as young men to testosterone's anabolic effects; however, older men have lower testosterone clearance rates, higher increments in hemoglobin, and a higher frequency of adverse effects. Although substantial gains in muscle mass and strength can be realized in older men with supraphysiological testosterone doses, these high doses are associated with high frequency of adverse effects. The best trade-off was achieved with a testosterone dose (125 mg) that was associated with high normal testosterone levels, low frequency of adverse events and significant gains in fat-free mass and muscle strength.
An other study (Yarrow et all 2011) concluded that low-dose administration of the non-5α-reducible androgen Trenbolone Enanthate maintains prostate mass and hemoglobin concentrations near the level of shams while producing potent myotrophic actions in skeletal muscle and partial protection against orchiectomy-induced bone loss and visceral fat accumulation. Our findings indicate that Trenbolone enathate has advantages over supraphysiological testosterone and supports the need for future preclinical studies examining the viability of Trenbolone Enanthate as an option for androgen replacement therapy
jgfjdl
hkdfkg
- Login to post comments