
how long does it take for testosterone to work

Objectives: Testosterone has a spectrum of effects on the male organism. This review attempts to determine, from published studies, the time-course of the effects induced by testosterone replacement therapy from their first manifestation until maximum effects are attained.
Design: Literature data of testosterone replacement
Results: Effects on sexual interest appear after 3 weeks plateauing at 6 weeks, with no further increments expected beyond. Changes in erections/ejaculations may require up to 6 months. Effects on quality of life manifest within 3-4 weeks, but maximum benefits take longer. Effects on depressive mood become detectable after 3-6 weeks with a maximum after 18-30 weeks. Effects on erythropoiesis are evident at 3 months, peaking at 9-12 months. Prostate specific antigen and volume rise, marginally, plateauing at 12 months; further increase should be related to aging rather than therapy. Effects on lipids appear after 4 weeks, maximal after 6-12 months. Insulin sensitivity may improve within few days, but effects on glycemic control become evident only after 3-12 months. Changes in fat mass, lean body mass and muscle strength occur within 12-16 weeks, stabilize at 6-12 months, but can marginally continue over years. Effects on inflammation occur within 3 to 12 weeks. Effects on bone are detectable already after 6 months while continuing at least for 3 years.
Conclusion: the time-course of the spectrum of effects of testosterone shows considerable variation, probably related to pharmacodynamics of the testosterone preparation. Genomic and non-genomic effects, androgen receptor polymorphism and intracellular steroid metabolism further contribute to such diversity.
Treatment of hypogonadal men with testosterone is rewarding, for the patients as well as the physician. The patient experiences, to his satisfaction, profound changes in his physical appearance and his mental make-up. The attending physician observes the changes the patient undergoes and rarely fails to be fascinated by the multitude of functions testosterone appears to have in the process of masculinization in the broadest sense 1.
While the effects of testosterone have been described in detail, relatively little attention has been given to the time these effects take to occur and achieve a full expression. This seems relevant. To the attending physician, monitoring the effects of administration of testosterone will be facilitated when it is known when certain effects can and should be expected. Patients like to receive information when the effects will set in. If patients have not been exposed to testosterone at the usual time of puberty, they must be prepared and counseled about the emergence of sexual thoughts and dreams, an increase in erections and seminal emissions, and when to expect them. Further, this information is relevant for the design of clinical trials on testosterone replacement therapy. It is important to have information when an effect can be expected and when its maximum has been attained.
METHODOLOGICAL SEARCH
Data to compile a time-course for the diverse actions of testosterone are not easily available. They originate from studies analyzing the effects of testosterone administration to hypogonadal men or, alternatively, from studies on androgen deprivation. The main source of information will be the former category. Nearly all of these studies were not specifically designed to address the onset or time-dependency of effects of testosterone, nevertheless a number of controlled studies with different design and scheduled follow-up, allow a reasonable estimation.
Studies were identified by a computerized search of MEDLINE, the Cochrane Library, EMBASE and Current Contents for the past 40 years (1976–2011), by searching the bibliographies of all retrieved articles and examining references of review articles.
There is now evidence that the spectrum of complaints of testosterone deficiency cannot be related to a specific threshold of testosterone concentrations, but that thresholds vary with the various symptoms of testosterone deficiency 2. In a cohort of men androgen-related loss of libido or vigor became more prevalent when testosterone concentrations fell below 15 nmol/liter, while depression and diabetes mellitus type 2 (also in non-obese men) were significantly more present in men with testosterone concentrations below 10 nmol/liter. Symptoms related to androgen deficiency in this study could be subdivided in three independent groups: psychosomatic complaints, metabolic disorders, and sexual health problems. Patients suffering from one of these three groups exhibit distinct features in terms of androgen levels, age, and body mass index. So, complaints are not only linked to androgen levels but age and body mass index carried weight as well in the manifestation of signs and symptoms of androgen deficiency 2. To further complicate the matter of the relationship between testosterone levels on the one hand and symptoms of testosterone deficiency on the other, there is the multifactorial impact on certain androgen-related functions 2. Erectile dysfunction may serve as an example of a composite dysfunctionality in which arterial endothelial function, neuronal integrity, testosterone concentrations, and psychological factors play pivotal roles 3, 4, almost precluding establishing a straightforward relationship between testosterone levels and erectile dysfunction. In a study only testosterone concentrations below 8 nmol/liter contributed to the symptom of erectile dysfunction 2.
Given that the clinical manifestations of testosterone deficiency do not occur at a definitive threshold value of circulating testosterone, but vary with the target organ, associated symptoms and underlying conditions, it is even more complicated to establish a time-course since a reversal of these symptoms of deficiency is not only dependent on restoring serum testosterone to normal. In fact, at least two new variables are to be entered into the model: pharmacodynamics of the testosterone preparation and pharmacogenomics of the treated subject. Indeed, if replacement therapy fails to restore idiosyncratic ‘adequate’ androgen levels, it also will fail to ‘reverse’ its clinical manifestations. The issue is that defining ‘adequate’ replacement will necessarily have a certain range of serum testosterone values.
A possible solution to this will be to replace ‘universal threshold’ with ‘percentage rise’ in circulating testosterone achieved under replacement therapy. The latter varies inversely with the starting concentration of testosterone and predicts the magnitude and rapidity of response to treatment. Thus, the less hypogonadal the subject, the larger the increase in circulating testosterone values must be for the effect to be ‘perceived’ by the subject, and the longer the duration of treatment to achieve an instrumentally measurable difference in the desired outcome5.
The time-course for the spectrum of effects of testosterone may vary considerably, as testosterone actions are exerted though a cascade of many different pathways. Most of the actions of testosterone take place via the androgen receptor as a transcription factor activated by testosterone. The bound androgen receptor acts as transcription regulatory element by binding to specific DNA response elements in target gene promoters, causing activation or repression of transcription and subsequently protein synthesis. Over the past two decades evidence of rapid responses to androgens, dependent or independent of the androgen receptor, occurring at the cellular and organ level has accumulated to implicate rapid responses to androgens. Androgen's rapid time course of action; its effects in the absence or inhibition of the cellular machinery necessary for transcription/translation; and in the absence of translocation to the nucleus suggest a method of androgen action not initially dependent on genomic mechanisms 6. Examples are actions of testosterone on the brain and on vascular tone 7.
In addition to the time course of the actions of testosterone on androgen-dependent biological variables, table 1 presents an indication of quantitative changes associated with testosterone administration.
TIME-COURSE OF EFFCTS ON MUSCLE MASS / STRENGTH
In a series of studies Bhasin and coworkers have demonstrated that upon testosterone administration, there is a positive correlation between blood testosterone concentrations and leg press strength, thigh and quadriceps muscle volume, and, further, levels of hemoglobin and IGF-1 8. In a later study the same group of authors concluded that the anabolic response to testosterone can largely be predicted by the dose administered 9. If the dose administered is too low, no effects may be demonstrable 10. Recent studies of the effects of testosterone on muscle mass/strength are mostly short term. In a study that combined testosterone with growth hormone, total lean body mass increased as did appendicular lean tissue. Composite maximum voluntary strength of upper and lower body muscles had increased after 16 weeks 11. A study investigating the effect of a 12-week long-acting testosterone administration on maximal exercise capacity and muscle strength found an increase in quadriceps isometric strength, maximal voluntary contraction and isokinetic strength (peak torque) 12. Testosterone administration for 20 weeks was associated with dose-dependent increases in skeletal muscle mass, leg strength, and power 13. In a study of 180 days of treatment with a 1% T gel preparation (50 or 100 mg/day, contained in 5 or 10 g gel, mean muscle strength in the leg press exercise increased by 90 days and had not improved further at 180 days 14. A study25, 26 similar in design found an increase in lean body mass and an improvement of lower limb muscle strength after six months 15. Another study using high doses of testosterone gel (starting dose 100 mg/day with possible up-titration to 150 mg/day) observed significant increases in leg-press strength, chest-press strength, and stair-climbing power with a load within 6 months 16. A study administering testosterone enanthate, 200 mg /2 weeks observed major effects to occur over the first 12 months of testosterone administration, thereafter minor increases could be observed 17. It can be concluded that the effects of testosterone on muscle strength are demonstrable after 12-20 weeks and that depending on the achieved testosterone levels, the maximum effects are attained after 6 months or 12 months. TIME-COURSE OF EFFECTS ON BONE MINERAL DENSITY
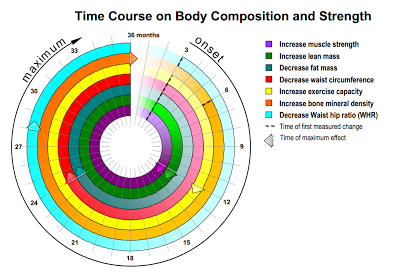
The effects of testosterone on bone mineral density are in part mediated by estrogens, derived from testosterone via aromatization 18. Testosterone improves bone mineral density at the lumbar spine compared to placebo, but at the femoral neck improvements are less certain 19. Testosterone produces a consistent reduction in bone resorption markers 20. Effects on bone mineral density have been shown in studies of six months duration 21, 22, eight months duration 23 or one year 24. From studies analyzing the effects of testosterone administration over as long as 36 months an increase was observed over that time period and it did not become clear whether the maximum effects of testosterone improving bone mineral. The data are summarized in figure 1.
TIME-COURSE OF EFFECTS ON BODY COMPOSITION
Testosterone plays a significant role in obesity, glucose homeostasis and lipid metabolism 27. At the cellular level there is now insight into the effects of androgen deprivation / administration on fat mass and muscle mass. Testosterone regulates lineage determination in mesenchymal pluripotent cells by promoting their commitment to the myogenic lineage and inhibiting their differentiation into the adipogenic lineage through an androgen receptor-mediated pathway. The observation that differentiation of pluripotent cells is androgen dependent provides a unifying explanation for the reciprocal effects of androgens on muscle and fat mass in men 28, 29. Upon testosterone administration there is a decrease of fat mass and an increase in lean body mass and the net result is often, but not always, that total body weight does not show major changes. An increase in total mass was found after three months 14 and an increase in weight in elderly men after three months 30. A decrease in weight has been observed after three months 31 and six months 17, with further progressive decrease over 24 months32. An increase in total body mass, lean body mass and a decrease in fat mass were found after three months 14 30 or six months 17. A decrease in fat mass has been widely reported after three months 31; 14 30 or six months 17, and a decrease in percent fat mass equally after three months 14 31.
It is now commonly accepted that a preferential accumulation of fat in the abdominal region is associated with an increased risk of type 2 diabetes mellitus and cardiovascular disease, not only in obese subjects but even in non-obese subjects 33. Therefore, the effects on trunk fat, often measured as changes in waist circumference 34, are very relevant effects of testosterone treatment. A decrease in trunk fat or waist circumference was noted in a number of studies after three months 35 36 with continuous decline over 24 months32 and a decrease in the waist hip ratio after three months 31 36 or after six months and 30 weeks, respectively.17 A continued decline up to 110 weeks was reported37. Body mass index as a widely used measure of body composition declined after 6 months with further improvement during an observation period of 2 years32. The data are summarized in figure 1.
TIME-COURSE OF EFFECTS ON LIPIDS
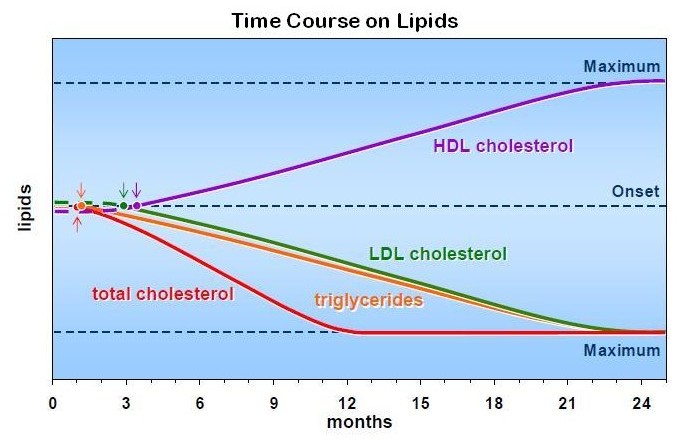
Decreases in serum total cholesterol have been noted as quick as after four weeks 38 39 but most studies have reported a decrease after three months 35 36. A decrease after 24 weeks was observed in a recent study 40, others have found this to occur after nine months 41 or 12 months 42 with a maximum reached after 12 months32 The decrease in serum triglycerides follows a similar pattern: after four weeks 38, after three months 35, and with further decrease over nine months 41 or12 months 43.
The decrease in low density lipoprotein cholesterol seems somewhat slower: after three months 35, after 40-44 weeks 44 or after 12 months 42 with a maximum observed after 24 months32.
Studies have found both an increase and decrease in high density lipoprotein cholesterol. An increase was found to occur after three months increasing further during 12 months 43, after six months 35 or close to one year 44. Continuous increase was seen over 24 months32.
TIME-COURSE OF EFFECTS ON GLYCEMIC CONTROL
Several studies indicate that upon testosterone administration serum glucose is lower after three months in men with impaired glucose tolerance 31 36 43. In a recent study this was observed after 24 weeks only in men with baseline glucose > 110 ng/ml (6.6 mmol/L) but not significantly in men whose baseline glucose levels were < 110 ng/ml (6.6 mmol/L).40 An early study reported a decrease in glucose and glucose disposal rate after 9 months 41.
A decrease in serum pro-insulin and insulin was noted after three months 43 or six months 45, and a decrease in HOMA after three months 36 or six months 45 46, 47. A decline in HbA1c was observed after three months 36, 43 31 with further decrease after 12 months 43.
Low serum testosterone levels are associated with an adverse metabolic profile which may be explained by the observation that low testosterone levels and impaired mitochondrial function promote insulin resistance in men48. And indeed, in an experimental study, stimulation of endogenous testosterone was shown to increase insulin sensitivity within 48 hours 49.
Recently, it has been demonstrated that the interplay between insulin sensitivity, is not facilitated by changes in body composition alone. Concomitantly increasing testosterone and decreasing E2 levels had positive effects on both postprandial triglyceride handling and insulin sensitivity in elaborate clamp models during manipulation of these serum sex steroid levels 50. The effects on postprandial triglyceride handling can therefore be seen in line with previous results and seem to be of relevance for metabolic risk 51, 52. An improvement in insulin sensitivity upon testosterone administration resulted in reduced fasting glucose and insulin levels within a single week 50, corroborating the former reports about an increase in insulin sensitivity upon stimulation of endogenous testosterone within 48 hours49 and an acute reduction in insulin sensitivity 2 weeks after discontinuing testosterone replacement in severely hypogonadal men 53.
Such observations are most likely attributed to testosterone-induced changes in lipid metabolism and/or altered post-receptor insulin signaling in muscle 54 and also improved insulin sensitivity enhancing muscle lipid uptake 55. Furthermore, the aforementioned intervention increased the response of postprandial glucose-dependent insulinotropic polypeptide (GIP) release 50. Effects of sex steroids on GIP had not been reported before. This is of specific interest, as action of GIP is not limited to pancreatic cells and may affect lipid homeostasis 56 and intestinal glucose transport 57.
TIME-COURSE OF EFFECTS ON BLOOD PRESSURE AND OTHER CARDIOVASCULAR EFFECTS
In some studies a decline in diastolic blood pressure has been observed, after 3-9 months 22 41 35, 44 and in some studies also in systolic blood pressure 35 44. Maximum effects were observed after 12 months35. A decrease in the resting heart rate occurred after 40-44 weeks 44. A decrease in arterial stiffness measured as pulse wave velocity was measurable after 48 hours 58 and in large artery compliance after three months 58. Several studies have been conducted in men with heart disease. In men with chronic stable angina pectoris the increase in time to 1 mm ST segment depression was noticeable after 14 weeks 59. The ischemic threshold had increased after four weeks 38. Exercise capacity in men with chronic heart failure increased after 12 weeks 60, whereas the cardiac index (cardiac output)14, 69, and related to body surface) had increased already after 180 minutes. In men with coronary artery disease flow mediated vasodilatation was observed after 12 weeks 61.
TIME COURSE OF EFFECTS ON INFLAMMATORY FACTORS / ENDOTHELIAL MARKERS
Low sex hormone levels are associated with inflammation 62 . Already after three weeks of testosterone administration, a decline was noted in IL-6 63 and in another study after 16 weeks 64. A decrease in C-reactive protein was observed after three weeks 63 and in other studies after three months 32, 43. In a study in patients with Crohn’s disease, CRP levels continued to decline over 24 months65. A decrease in tumor necrosis factor alpha and in interleukin 1-beta was noted after 4 weeks 39. Asymmetric dimethylarginine is a endogenous NO synthase inhibitor and appears to decline upon testosterone administration after 10 days 66 or after 4 weeks 67.
TIME-COURSE OF EFFECTS ON SEXUAL PARAMETERS
• Effects on libido
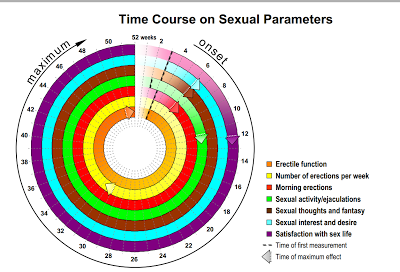
Effects on libido, sexual desire, sexual thoughts and fantasies and satisfaction with sexual life manifest themselves rather rapidly: after three weeks 68 or 30 days 14. Some studies have measured these effects only after three months 31
• Effects on erection /ejaculation
Effects on erection appear also rather rapidly: after 3 weeks 68. Increase in morning erections occur after three weeks 68. An increase in percentage of full erections and sexual performance and satisfaction with erections was noticed after 30 days increase of ejaculations and sexual activity after two weeks70 and three weeks, respectively 68. In patients with veno-occlusive dysfunction, testosterone undecanoate restored erectile function after a minimum of 3 months and a maximum of 11.5 months71.
The International Index of Erectile Function is a reliable, self-administered measure of erectile function that is cross-culturally valid and psychometrically sound, with the sensitivity and specificity for detecting treatment-related changes in patients with erectile dysfunction. It has five domains: erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction. Increases in the IIEF erectile function have been noted after three months 35 40 but increases in IIEF sexual desire, intercourse satisfaction and overall satisfaction appear already after 6 weeks 40. Maximal effects are usually achieved after 3 to 6 months72 but may take even up to 1 year in individual cases71. The data are summarized in figure
TIME-COURSE OF EFFECTS ON QUALITY OF LIFE
The St. Louis University Androgen Deficiency in Aging Male (ADAM) is a screening tool for hypogonadism in older males. An improvement was noted after one month of testosterone treatment 38. The Aging Males’ Symptom (AMS) questionnaire is a 17-item scale assessing health related quality of life and symptoms in aging men (e.g., somato-vegetative, psychological, and sexual symptoms) 73. Improvements on scores on the AMS have been noted after one month 38, six weeks 40 to three months on treatment with parenteral testosterone undecanoate 35 or after nine months on testosterone gel 74 continuing over a total of 18 months 74.
TIME-COURSE OF EFFECTS ON PSYCHOLOGICAL VARIABLES
Several studies report an improvement of depression after three weeks 68 or one month 38. Increase in good mood and a decrease in bad mood were noted after three weeks 68 or after 30 days 14. There also was an increase in motivation after 30 days which was maintained thereafter 14. Two studies using the Hamilton Depression Rating Scale found an improvement of depression after six weeks 75 or eight weeks 76. A number of psychological variables (increase of sociability, decrease of anxiety, increase in concentration and self-confidence) were apparent after three weeks 68. A decrease of fatigue and listlessness was found after one month 31 or six weeks 68. A transient increase in anger / hostility was found in eugonadal men whose testosterone levels were raised above normal after two weeks 77.
In a larger set of severely depressed men (n=2x50), effects of TRT by gel vs placebo were seen within 6 weeks. The effect was not consistent within the whole group of patients. It is likely that, in severe clinical depression, the receptiveness for testosterone effects depends on the overall pattern of disturbed neurotransmitters, especially noradrenaline and serotonine, and also baseline testosterone concentrations78. It is very likely that the positive effects of testosterone on depressive symptoms start as early as after 3 to 6 weeks, but will most likely take 18 to 30 weeks to find the patient with a significant improvement. A recent study in hypogonadal men receiving testosterone undecanoate i.m. demonstrated such effects. It is remarkable that effects were more pronounced in men with lowest baseline testosterone levels 79.
Likewise, effects of testosterone administration in hypogonadal men on the ability to process spatial data of visual content were seen within 2 weeks of treatment 80. These effects are obviously directly related to testosterone and not its aromatization product estradiol, as it was later confirmed in a placebo-controlled trial involving an aromatase inhibitor combined with testosterone administration in hypogonadal men. These patients exhibited a markedly improved spatial working memory within 3 weeks, improving further until week six 81.
TIME-COURSE OF EFFECTS ON ERYTHROPOIESIS
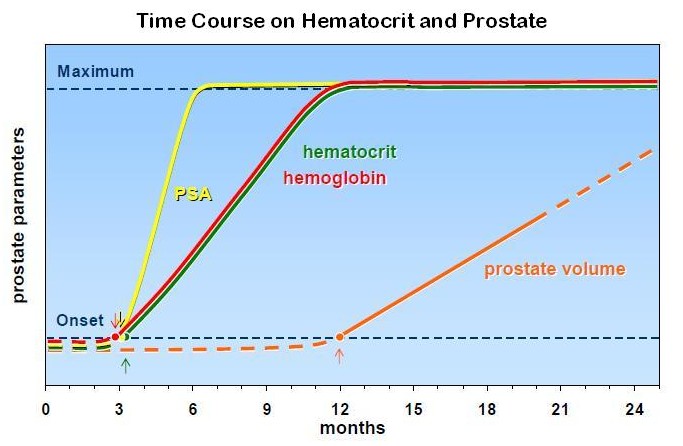
The effects of testosterone on red blood cell formation (hemoglobin and hematocrit) are dose dependent 82 14 83 while higher age is also a factor 44. The effects are apparent after 3 months 14 40 35 and a maximum is reached after 9- 12 months 35.
TIME-COURSE OF EFFECTS ON THE PROSTATE
In hypogonadal men treated with testosterone, levels of prostate specific antigen (PSA) rise, usually up to levels of eugonadal men 84. Upon judging the time course of effects of testosterone on the prostate, it is of note that aging itself is a factor in the rise of both prostate volume and PSA 84, and there is no endpoint in the effects of testosterone on the prostate. A rise in PSA levels was noticed after six months, whereafter over the following 24 months there was no significant further increase 85. Other studies have found a rise of PSA levels after three months 40, some only after after 12 months 43. An increase in prostate volume was noted after 3 months86 and after 12 months 44. One study over 24 months found no significant increases of both PSA and prostate volume. In a study of 123 subjects over 42 months of testosterone gel application, there was significant increase of serum PSA over the first six months and then no further significant increases with continued testosterone treatment was found 87. In a study of 81 hypogonadal men (mean age 56.8 years) followed for a mean (range) of 33.8 (6-144) months PSA levels did not increase significantly at 1-year intervals for 5 years 88.
DISCUSSION
This is a systematic analysis of the time-course of the spectrum of biological effects of testosterone on the various target systems. The authors view this as a worthwhile endeavor for a number of reasons. Attending physicians can prepare their patients what the time periods are after which to expect effects of testosterone. Studies investigating the effects of testosterone have to take this time course into consideration to design the duration of studies to be able to have quantifiable measurements.
It is of note that almost none of the quoted studies had been specifically designed to assess the time course of effects. Some studies measure effects of testosterone only after three months 31, and, particularly, effects on libido and erections have occurred well before this time span
We noticed considerable differences in the occurrence of effects of testosterone. Effects on libido and other psychological variables and effects on vasculature occur 32, 35, 92 rather rapidly. It may well be that these effects are not mediated via the classical androgen receptor but through other mechanisms like effects on membranes 6 7. Also effects on erection occur rather rapidly and may be partially explained by non-genomic effects on vascular penile erectile tissue 89
The effects of testosterone on glycemic control and variables clustered in the metabolic syndrome occur somewhat slower, but there is evidence that acute testosterone fall during deprivation therapy is directly related to a worsening in insulin sensitivity 53. However, in a recent study the authors were not able to substantiate their earlier finding 90 and hypothesize insulin resistance associated with chronic low testosterone levels may be largely driven by decreased fat free mass, increased percent body fat, and/or other metabolic regulatory factors. This may apply also to other factors of the metabolic syndrome. Testosterone inhibits the expression of the activity of lipoprotein lipase, the main enzymatic regulator of triglyceride uptake in the fat cell, preferentially in abdominal fat 28, 29. Several studies have indeed confirmed that testosterone treatment reduces waist circumference which, in its simplicity, appears to be a valid parameter of the degree of visceral obesity 91. In our own studies, signs and symptoms of the metabolic syndrome improved substantially following administration of long-acting testosterone undecanoate and improvements in glycemic control andlipids paralelled improvements in body composition.
The effects of testosterone on muscle and bone involve protein synthesis and are a result of genomic actions of testosterone and, therefore, rather slow.
Apart from reviewing the onset of effects of testosterone treatment in hypogonadal men, it would also be possible to look at the onset of symptoms of testosterone deficiency in patients on androgen deprivation therapy (ADT), standard treatment for men with advanced prostate cancer. ADT causes unfavourable changes in body composition, insulin resistance and other risk factors for cardiometabolic diseases leading to an increased incidence of cardiovascular diseases and type 2 diabetes (for review93, 94). However, deprivation of testosterone and the time-dependent effects thereof might be totally different from the onset of testosterone action in testosterone treatment, even in the same parameter. It was therefore decided to restrict this paper to aspects of testosterone treatment.
Finally, in the present analysis it was attempted to select those studies of testosterone treatment that provided adequate doses/ delivery of testosterone. It is obvious that sub-optimal therapeutic regimens or, alternatively, inappropriate patient selection (eugonadal or men with biochemical but not clinical hypogonadism) may show different time-course of effects.
In conclusion: this analysis tries to chart the differences in time periods after which biological effects of testosterone administration in hypogonadal men occur. This may add to a better understanding of the physiology of androgen action. Earlier studies have shown that there are thresholds for the various actions testosterone: in other words signs and symptoms of testosterone deficiency appear at different threshold values of circulating testosterone. The above results call for a well designed study that charts the time required to restore an androgen dependent function with the optimal circulating testosterone for that specific androgen-dependent function. These studies are not easy to perform. Ideallly, they should measure at what serum levels of testosterone, all androgen-dependent biological functions are restored. Some biological functions, like erectile functions are composite in nature, and next to testosterone, endothelial function and psychological factors are equally relevant2. A major problem is the so-called late onset hypogonadism: the decline of serum testosterone with aging. It is still hotly debated whether this is a true form of hypogonadism, or a decline of serum testosterone associated with the progressive accumulation of health problems with aging95, 96, but rather independently of the process of aging itself. Though small-scale studies show benefits and acceptable risks of treating elderly men with lower-than-normal testosterone levels46, 97, a verdict can only be reached with large-scale studies including 5000 men over 5 years95, for which presently the funding is not available. There is a degree of consensus that elderly men with serum testosterone clearly below the reference ranges and persistent clear clinical signs of hypogonadism may justifiably be treated98, 99, but there remains a large degree of dissent.
- Login to post comments