
Female sexuality and well being

Faithful readers of this blog know that made many blogposts about the influence of Testosterone on libido as well as hypogonadism on men. But it takes two to tango. Thus lets focus on the women in this regard. Don’t be mistaken women, just like men, use all kinds of drugs to start, restore, maintain or enhance their libido, especially when growing older.
Although sexuality remains an important component of emotional and physical intimacy that most men and women desire to experience throughout their lives, sexual dysfunction in women is a problem that is not well studied. The prevalence of sexual dysfunction among all women is estimated to be between 25% and 63%; the prevalence in postmenopausal women is even higher, with rates between 68% and 86.5%. Increasing recognition of this common problem and future research in this field may alter perceptions about sexuality, dismiss taboo and incorrect thoughts on sexual dysfunction, and spark better management for patients, allowing them to live more enjoyable lives. It is expected that the United States’ older population, those persons age 65 and above, will grow substantially as the Baby Boom generation ages.
This predicted change in our demographics creates an even greater need for a thorough understanding of issues affecting the elderly. This need is especially acute for physicians who will increasingly encounter patients trying to maintain a high quality of life as their bodies and life circumstances change, and as advances in nutrition, health maintenance, and technology allow many to extend the time midlife activities are maintained.
O ne quality-of-life issue affected by these changes, for both men and women, is sexuality. Although studies agree that the majority of women consider sexuality a very important determinant of quality of life, the literature on the subject of sexual function in elderly women is not extensive. In addition to being sparse, the existing literature employs varying approaches, encompasses differing foci, and illustrates contradictory results on sexual function in the elderly population.
ne quality-of-life issue affected by these changes, for both men and women, is sexuality. Although studies agree that the majority of women consider sexuality a very important determinant of quality of life, the literature on the subject of sexual function in elderly women is not extensive. In addition to being sparse, the existing literature employs varying approaches, encompasses differing foci, and illustrates contradictory results on sexual function in the elderly population.
Treatments for women's libido issues are an untapped financial opportunity for drug makers. Analysts estimate the market could be worth over $2 billion, based on academic estimates that between 5 million and 9 million U.S. women may suffer from desire disorders.
Testosterone therapy is of growing interest because of its increasingly recognized role in sexual and mental health, bone and muscle trophism and vitality. An expanding body of evidence supports the influence of testosterone on sexuality, with the focus on desire and central (mental) arousal.
T he neurobiology of sexual desire and central arousal and the peripheral neurovascular response are substantially modulated by sexual hormones.
he neurobiology of sexual desire and central arousal and the peripheral neurovascular response are substantially modulated by sexual hormones.
Androgens have a leading role in the initiation and modulation of sexual function, in women as well as in men. In men, testosterone is 10 times higher than in women, contributing to the stronger intensity of the male sex drive. Multiple neurotransmitter systems in the brain, especially the areas known to regulate mood and desire (including the amygdala, hippocampus and hypothalamus), are heavily influenced by sex hormones. The serum levels of testosterone and of pro-androgens exceed those of oestradiol, even during the peak reproductive years
While doctors are slowly recognizing the benefits of testosterone therapy for aging men, evidence that women also become testosterone deficient is largely ignored. Controlled studies show that slightly increasing testosterone levels in aging women restores sexual drive, arousal, and frequency of sexual fantasies. In fact, low testosterone levels in women of all ages seem to suppress libido and cause sexual dysfunction. Restoring youthful testosterone in women has been shown to improve mood and well-being, and to provide many other health-enhancing benefits.
==========================================================================
 Alessandra Graziottin, the MD Director of the Center of Gynaecology and Medical Sexology from Milan, Italy, did a lot of studies towards the effects of androgens on women.
Alessandra Graziottin, the MD Director of the Center of Gynaecology and Medical Sexology from Milan, Italy, did a lot of studies towards the effects of androgens on women.
From her study Androgen effects on the female brain , this excerpt and conclusions:
For decades, research on the role of sexual hormones on women’ and female animal brain has been focused on estrogens, with scant data on androgens (testosterone, androstenedione, dehydroepiandrosterone sulfate/DHEA-S), in spite of the fact that the serum levels of testosterone and of pro-androgens exceed that of estradiol, even during peak reproductive years. Only in the last decade the focus has definitely shifted on the role of androgens.
Androgens have a powerful trophic and reparative effect on neurons and glial cells via a direct (membrane, non-genomic) and indirect (genomic) mechanism of action. Testosterone effects are either via the Dehydrotestosterone (DHT) and the AR; via estrogen and the ER, after aromatization; or via conversion of DHT to 3α-diol and non-genomic signals (GABA-A receptors). Their effect on neuroplasticity is the biological correlate of psychoplasticity, a key issue when considering the current concern on women’s brain aging. As androgens peak at 20s, are halves at 40s with a further decline with increasing age, the issue of the impact of this loss on the brain if of the highest importance, more so in women who underwent bilateral oophorectomy during the fertile age. The evidence on the effects of testosterone and DHEA-S on the female brain is still scant. Specific concern is raised by the long term effect on women’s brain and mental functions of aromatase treatment in breast cancer survivors. The evidence is surprisingly lacking.
Systems and functions where testosterone have a definite role include:
a ) the cholinergic system, involved in cognition and memory: difficulty concentrating is negatively correlated with testosterone. Women who underwent oophorectomy before the onset of menopause had an increased risk of cognitive impairment or dementia compared to referent women, adjusted for education, type of interview, and history of depression). The risk increases with younger age at oophorectomy.
) the cholinergic system, involved in cognition and memory: difficulty concentrating is negatively correlated with testosterone. Women who underwent oophorectomy before the onset of menopause had an increased risk of cognitive impairment or dementia compared to referent women, adjusted for education, type of interview, and history of depression). The risk increases with younger age at oophorectomy.
b) the serotoninergic system, involved in mood: estrogen and add-back testosterone have both been shown to positively affect mood and well-being.
c) the dopaminergic system, involved (also) in neuromotor competence, the system most neglected when discussing women’s brain: the risk of parkinsonism increases following oophorectomy), with a borderline significance for Parkinson’s disease. In particular, there is a linear trend of increasing risk with younger age at oophorectomy.
Androgens have a powerful effect in boosting women’s sexual function. Neurobiology of sexual desire and central (mental) arousal, and the peripheral neurovascular response are substantially modulated by sexual hormones. Androgens have a leading role in the initiation and modulation of sexual function, in women as in men. In men they are ten times higher than in women, contributing to the stronger intensity of sex drive in men. Multiple neurotransmitter systems in the brain, especially the areas known to regulate mood and desire (including the amygdala, hippocampus and hypothalamus) are heavily influenced by sex hormones.
Testosterone specifically increases physical and mental energy (which potentiate sexual desire), assertiveness and lucidity; stimulates mental and genital sexual arousal, erotic dreams, voluntary and spontaneous sexual fantasies; increases nipple and genital excitability, of the clitoris and cavernous bodies; reduces the lag-time between the beginning of the fore-play and the achievement of orgasm with a central and peripheral mechanism; increases the intensity and pleasure of orgasm and facilitate the achievement of multiple orgasms.
Conclusion The women’s brain is a key target of testosterone. All brain functions are modulated by androgens. More research is needed to substantiate the role of androgens on neurons and glial cells and the complex benefits appropriate androgen replacement may offer women who want to age mentally at their best.
=========================================================================== Patches – Creams and Plasters
T he 2014 study: Pharmacokinetics of a transdermal testosterone cream in healthy post -menopausal women, came to the conclusion: “One percent TTC (formulated as AndroFeme), when applied daily as a 5-mg dose to the upper arm of naturally postmenopausal women not using concurrent systemic hormone therapy, restores TT and fT levels to levels above and within the reference range, respectively, for premenopausal women”
he 2014 study: Pharmacokinetics of a transdermal testosterone cream in healthy post -menopausal women, came to the conclusion: “One percent TTC (formulated as AndroFeme), when applied daily as a 5-mg dose to the upper arm of naturally postmenopausal women not using concurrent systemic hormone therapy, restores TT and fT levels to levels above and within the reference range, respectively, for premenopausal women”
Testosterone is best utilized when applied in its cream or gel form to the inner thigh, buttocks, small labia or the non-hairy area between the vagina and rectum called the perineum.
W omen with low testosterone levels who attach an Intrinsa testosterone plaster to their body become more muscled and feel better, according to a study by researchers at Massachusetts General Hospital. They tested the plasters for a year on 25 women with hormonal abnormalities.
omen with low testosterone levels who attach an Intrinsa testosterone plaster to their body become more muscled and feel better, according to a study by researchers at Massachusetts General Hospital. They tested the plasters for a year on 25 women with hormonal abnormalities.
Intrinsa is made by Procter & Gamble. The women stuck two plasters on their abdomen and changed them twice a week. The plasters provided the women with 150 micrograms of testosterone every day. This dose is only six percent of the amount of testosterone provided to men when they use this kind of patch.
T he researchers did a trial on fifty women between the ages of 19 and 50 whose sexual organs and adrenals no longer produced testosterone because their hormone glands in the brain were not functioning properly.
he researchers did a trial on fifty women between the ages of 19 and 50 whose sexual organs and adrenals no longer produced testosterone because their hormone glands in the brain were not functioning properly.
Their free testosterone level was 0.5 – 0.6 pg/ml. Normal values are 1.1 – 6.3 pg/ml. The testosterone level of the 25 women who were given Intrinsa plasters returned to normal, as the figure left shows. The other half of the women were given a placebo.
What the figure doesn't tell is that a doctor regularly checked the women's hormone levels. Nine of the women had to halve their dose because their testosterone level rose too high. That's one in three of the test subjects.
The Intrinsa users' bone mass also increased, and the women using the Intrinsa plasters reported feeling better and found an improvement in their sex lives.
And, last but not least, the women's fat free mass increased, part of which was muscle mass.
T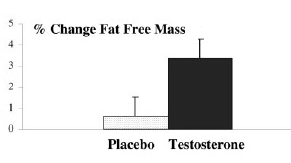 he women experienced hardly any side effects. The cholesterol levels of a few rose, but only by minimal amount. The most noticeable side effect was that eight women developed acne, the researchers reported.
he women experienced hardly any side effects. The cholesterol levels of a few rose, but only by minimal amount. The most noticeable side effect was that eight women developed acne, the researchers reported.
But we got hold of the table of side effects, and we noticed one that women might find interesting, even though it's not statistically significant. Seven women who used the Intrinsa plasters developed hirsutism (excessive hair growth).
Testosterone plaster (Intrinsa) BBC report on Intrinsa, the new "female Viagra" patch
===========================================================================
A risky aphrodisiac
At its launch it was already clear: only a minority of women who take Addyi, feels a (albeit very modest) "positive" effect on their libido. Sometimes serious side effects as possible. Recently a meta-analysis of all studies on the incentive effect on the libido of flibanserin was published. Flibanserin (the active ingredient of Addyi), was originally developed as an antidepressant. On average, this drug provides an additional half (!) satisfactory sexual intercourse per month possible, in comparison with a placebo. Adverse side effects can be: drowsiness and fatigue, but also sudden drops in blood pressure and loss of consciousness - especially in combination with alcohol or other drugs.
effects as possible. Recently a meta-analysis of all studies on the incentive effect on the libido of flibanserin was published. Flibanserin (the active ingredient of Addyi), was originally developed as an antidepressant. On average, this drug provides an additional half (!) satisfactory sexual intercourse per month possible, in comparison with a placebo. Adverse side effects can be: drowsiness and fatigue, but also sudden drops in blood pressure and loss of consciousness - especially in combination with alcohol or other drugs.
All this is food for thought. It is clear that the pharmaceutical industry (Big Pharma) overly medicalized female sexuality and exaggerate the virtues of their drugs, while minimizing the risks and flood us with "information campaigns" whose only real purpose is to maximize sales. In the words of the CEO of the Canadian group Valeant Pharmaceuticals, which has bought the laboratory Sprout which develloped Addyi: "We are confident that this product will bring hundreds of millions of dollars" ...
An example: Every night before Amanda Parrish and her husband Ben go to bed, she pops a little pink pill. She is taking the revolutionary new pill for women called Addyi, the "Female Viagra." She claims her sexlife is 'Like Teenagers in Heat.'
===========================================================================
Proviron – Anavar and Winstrol
A nabolic steroids can be very damaging to women as they can often cause masculine effects due to virilization, such as deepened vocal chords, body-hair growth and clitoral enlargement. When a woman takes anabolic steroids she can expect a massive libido boost. Most women prefer the oral anabolic steroids.
nabolic steroids can be very damaging to women as they can often cause masculine effects due to virilization, such as deepened vocal chords, body-hair growth and clitoral enlargement. When a woman takes anabolic steroids she can expect a massive libido boost. Most women prefer the oral anabolic steroids.
Due to its mild nature Anavar (oxandrolone) appears to be virtually side-effect free not only for men but for women as well, making it the ultimate anabolic steroid for any female user. While this steroid can be used successfully by both men and women, because it is so female friendly many refer to Anavar as “The Girl Steroid.” Anavar for women is as testosterone for men, safe and effective. There is no anabolic steroid better received than Anavar for women. Its however advised to take 10 mg per day, and that’s mostly all they need.
Female athletes should use Proviron (mesterolone) with caution since possible androgenic side effects cannot be excluded. Women who want to give Proviron a try should not take more than one 25 mg tablet per day. Higher dosages and periods of intake of more than four weeks considerably increase the risk of virilization symptoms. Female athletes who have no difficulties with Proviron obtain good results with 25 mg Proviron. Proviron is also very powerful increasing the libido, I wrote about it here.
Proviron is an extremely powerful hardening agent in a female. Women who struggled with estrogenic fat storage, especially on the legs reported noticing improvements in the quadriceps within 2 days of the addition of Proviron. Like Anavar, Proviron is easy on the liver and not likely to cause much toxicity, if at all. Proviron is not very anabolic, but is a useful antiestrogenic compound. Proviron provides a hard, quality look to muscle, and an overall improvement in the look of the female physique.
Although 12.5-25 mgs per day is a tolerable dose which should not produce intolerable negative side effects, virilization will become a concern if used in higher dosages by a female. Again, caution should be taken when increasing any dose.
Although women experience a few side effects due to Winstrol (stanonzolol) intake, it is one of the safest anabolic drugs that they can use. Winstrol has some positive side effects in women, which include an enhanced feeling of wellness, increase in strength, and decrease of estrogenic f at that is stored in the thighs, buttocks, upper arms, and abdomen. Some women also experience a heightened sex drive and quick recovery periods after workouts.
at that is stored in the thighs, buttocks, upper arms, and abdomen. Some women also experience a heightened sex drive and quick recovery periods after workouts.
Winstrol has lower androgenic qualities, which makes it the most preferred anabolic steroid for female athletes. Ideally, women should limit their Winstrol intake to 10mg a day or 20 mg every other day. This is a safe dosage level that women can take either orally or through injections. Women who have not taken any anabolic drug earlier including Winstrol should start their cycle with the lowest dose of 5 mg per day. The drug can be used safely for a period of six weeks after which some women may start experiencing side effects.
Women athletes should ideally restrict their dosage of Winstrol to 10 mg per day. However, some women may be able to tolerate as much as 20 mg every other day, although this kind of intake can increase the possibility of virilization in them, as stated above. When taking steroids as powerful as Winstrol, women should always exercise caution to prevent side effects. It is best to discontinue your dosage of Winstrol as soon as you experience any of the side effects. Otherwise, there is a risk that these effects may become permanent.
===========================================================================
FORIA Many women already knew that cannabis oil provides a delicious viagra effect in women. Apparently the creators of Foria came with a better idea.
I n 2014 they brought a lubricant for women on the market that can make women not only high, but also very very happy. It's also true, the cannabinoids in marijuana, can cause women to experience great orgasms
n 2014 they brought a lubricant for women on the market that can make women not only high, but also very very happy. It's also true, the cannabinoids in marijuana, can cause women to experience great orgasms
In the past women bought cannabis oil or made a suitable oil themselves. But now you can save yourself this trouble, because Foria is a ready-made lubricant for women where a cannabis concentrate is added. Foria is a lubricant on the basis of coconut oil, and a vial contains approximately 360 milligrams of cannabinoids. The product is 100% natural, and it is no problem if you accidentally (or on purpose ) swallow some.
The 44-year experience expert Stacy : "After using Foria, not only did I have multiple orgasms in a short amount of time, I experienced a deep relaxation in my mind, body and soul."
Using Foria
According to the manufacturer from the web site Foria, spray for best results 4 to 8 times on the clitoris, the inner and outer labia and the vagina. Every time you press, it sprays about 2 milligrams of THC. After 15 to 30 minutes the stuff starts to work, the website reports that you can use this time as foreplay.
=========================================================================== Nowadays many girls use peptides. Melanotan II (MT II) is an injectable peptide that will give you a nice dark tan without getting out in the sun for any length of time. One of its side effect is the increase in (male and) female libido. Not just the increase in sexual arousal - but an increase in the desire for sex.
This side effect is so pronounced that researchers isolated the cause of the increase in libido, and developed a female sex peptide Bremelanotide (PT141). Real hard-core users are snorting these peptides like coke…. More on this later..
