
Estrogen suppression

Estrogen suppression by aromatase inhibitors
 There are many articles published about the different compounds used to suppress estrogen. There are two primary estrogens, estradiol and estrone, with estradiol (E2) being the more active of the two forms
There are many articles published about the different compounds used to suppress estrogen. There are two primary estrogens, estradiol and estrone, with estradiol (E2) being the more active of the two forms
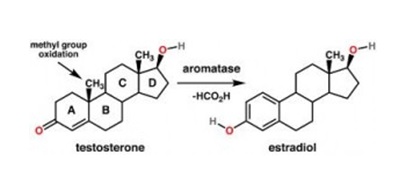
Aromatase is a complex of enzymes that convert the androgens testosterone, androstenedione ( and anabolic steroids) into estrogenic hormones
Not too long ago it was very simple, you just used a SERM like Nolvadex or Clomiphene. Many guys didn’t even use them, and just balanced with anabolic and androgenic compounds in their cycle. And with aromatizing and non-aromatizing compounds like Primobolan etc where popular.
 If you are doing a moderate cycle of 500 mg per week with a moderate oral you probably don’t need an aromatase inhibitor (AI) at all. On bigger doses normal Nolvadex and or Proviron should be sufficient. They have been for years. If you have a high level of testosterone, (because you inject or swallow anabolic steroids) the also higher level of estrogen is producing an anabolic effect. No need for aromatase inhibitors, unless of course you are developing side effects such as water retention, gynecomastia (the formation of female breast tissue) or benign prostatic hyperplasia. For the more advanced bodybuilder an aromatase inhibitor or better a combination of SERMs and an aromatase inhibitor is possible. Its advisable to inform yourself in that case, because new research shows new insight. Also the bro-science and pure nonsense on this subject on the internet and in the discussion forums are overwhelming. Also because some data stem from research on in postmenopausal women. Later in this post you will see how much those numbers can differ from those on healthy young men.
If you are doing a moderate cycle of 500 mg per week with a moderate oral you probably don’t need an aromatase inhibitor (AI) at all. On bigger doses normal Nolvadex and or Proviron should be sufficient. They have been for years. If you have a high level of testosterone, (because you inject or swallow anabolic steroids) the also higher level of estrogen is producing an anabolic effect. No need for aromatase inhibitors, unless of course you are developing side effects such as water retention, gynecomastia (the formation of female breast tissue) or benign prostatic hyperplasia. For the more advanced bodybuilder an aromatase inhibitor or better a combination of SERMs and an aromatase inhibitor is possible. Its advisable to inform yourself in that case, because new research shows new insight. Also the bro-science and pure nonsense on this subject on the internet and in the discussion forums are overwhelming. Also because some data stem from research on in postmenopausal women. Later in this post you will see how much those numbers can differ from those on healthy young men.
Breast cancer research has been extremely valuable. Breast cancers are typically responsive to female sex hormones (estrogens and progesterone). Therapies that reduce estrogen levels in the body and especially in tumors, have been actively investigated and developed by the pharmaceutical industry. This has resulted in the development of effective anti-aromatase drugs. Several drugs in this class have been developed.
Though most research on these drugs relates to breast cancer therapy, there have been several interesting studies on aromatase inhibition in human males.
De Ronde et al 2011: Over the past 15 years it has become evident that in men estradiol is responsible for a number of effects originally attributed to testosterone. Estradiol has an important role in gaining and maintaining bone mass, closing of the epiphyses and the feedback on gonadotropin secretion.
As estrogen is the principal factor responsible for epiphyseal fusion, aromatase blockers are being studied in the treatment of severe short stature in boys. This class of compounds has a theoretical advantage over using LHRH analogs to delay puberty, because they allow for progressive virilization while decreasing estrogens, potentially extending the time of epiphyseal fusion and thus the time for linear growth.
There's a recent opinion developing that prostate cancer has more to do with estrogen than with dihydrotestosterone, the theory being that many men, as they age, convert too much testosterone to estrogen and that this excessive estrogen is the cause of prostate enlargement or prostate cancer.
The Need for Estrogen Maintenance
Estrogen has both positive and negative effects that you should be aware of. On the positive it supports good high density cholesterol, enhances growth hormone output, increases muscle glucose utilization for tissue growth and repair, and even increases androgen receptor concentrations in various tissues. It is now understood that estrogen serves many useful purposes in men, particularly if we are looking for rapid muscle mass gain. If bulk is the goal it is therefore usually advised to hold off on estrogen maintenance compounds until there is a clear need for them. A certain amount of estrogen is necessary and can greatly aid size and strength gains. Men also need estrogen to maintain bone density, cognitive function, and even to maintain the inner lining of the arterial wall (the endothelium). And if your estrogen is suppressed to much your sex drive and your ability to get an erection is vanished, in a similar way low testosterone will work. Typical other sides include stiff joints and possibly lethargy, this may show you that you use to much aromatase inhibitor.
This brings us to the negative side of estrogen, namely that it can work to hide muscle definition by increasing water retention and fat buildup. It can also promote gynecomastia (the development of female breast tissue) in men if levels get too high. Since androgens and estrogens playing opposing roles on the disposition of body fat and the growth of mammary tissues, maximizing the ratio between these two hormones is often an important objective, particularly at times when dieting and cutting are key goals or gynecomastia is a worry because strongly aromatized hormones such as testosterone are being supplemented
Aromatase activity has not only been demonstrated in gonads and placenta but also in brain, fat tissue, muscle, hair, bone and vascular tissue.
Aromatase inhibitor letrozole downregulates steroid receptor coactivator-1 in specific brain regions that primarily related to memory, neuroendocrine and integration. Chen et all 2014
In this study Hippocampal estradiol, AR (androgen receptor), ERα (estrogen receptor) and ERβ were down-regulated by letrozole. Brain SRC-1 (steroid receptor coactivator-1) has multifunctional potentials in the mediating of steroids action. It may mediate letrozole regulation of memory, neuroendocrine and integration. The side effects of letrozole on CNS should be taken to serious consideration. Further research will without a doubt reveal of these side-effects also are true for other aromatase inhibitors
Nolvadex
Nolvadex (tamoxifen) works synergistically with Aromasin. You can find that on the net, so I won’t go into detail here. But Nolvadex kinda rejunivates your blood vessels by improving their elasticity. It also improved the blood lipids (HDL). A small protection against a heart attack, since you know roids are harsh on your blood lipids.
Hypogonadism
 There is a growing interest in the treatment of so-called late-onset hypogonadism, another name for the study of testosterone deficiency in an older age group.
There is a growing interest in the treatment of so-called late-onset hypogonadism, another name for the study of testosterone deficiency in an older age group.
Initial attempts at TRT/HRT testosterone replacement or hormone replacement therapy, have also brought attention to the possible adverse effects on the patients' cardiovascular risk factors and their prostate health. Aromatase inhibitors may be an attractive alternative for traditional testosterone substitution in elderly men because these compounds can be administered orally once daily and may result in physiological 24 h testosterone profiles. Additionally, misuse of aromatase inhibitors is unlikely since testosterone levels will not be stimulated to vastly supraphysiological levels.
Although aromatase inhibitors increase FSH levels, there is no consistent evidence for a beneficial effect on spermatogenesis. In older men with late-onset hypogonadism, aromatase inhibitors may emerge as an attractive alternative for traditional testosterone supplementation to improve testosterone levels. The long-term benefits of higher testosterone levels in older men remain controversial.
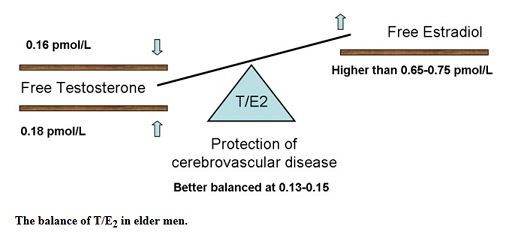
The “female” hormone estradiol is no longer considered as the feminizing hormone, as it has been identified to have an effect on the sexual and general well-being of adult males. Urologists and endocrinologists alike have started to pay attention to the serum T/E2 (testosterone : estradiol) ratio that appears to be more important than the respective individual hormonal levels. Therein lies the possible role of aromatase inhibitors (AIs) in restoring the normal balance of serum testosterone and estradiol levels for the adequate treatment of late-onset hypogonadism, while limiting the potential adverse effects.
Currently there is no literature to recommend the use of AIs in adult males to treat late-onset hypogonadism, obesity-related hypogonadotropic hypogonadism, gynecomastia, or male subfertility, although some positive effects have been reported. The adverse effects on bone health seen in females treated with AIs are not seen in males.
Clinical Use of Aromatase Inhibitors in Adult Males. Tan et al. 2014
Elevated t/e2 ratio is associated with an increased risk of cerebrovascular disease in elderly men. Gong et al. 2013
Most of us forget that once they will getting older too. The ones that have done some serious cycling at young age, will probably never get their natural (endogenous) testosterone level back. Then they will either be forced to start taking testosterone for TRT. Or take aromatase inhibitors like Aromasin to adjust their hormones.
A small, controlled study demonstrated that anastrozole in a dose of 1 mg daily during 12 weeks will result in doubling of the mean bioavailable testosterone level in older men. Aromatase inhibitors are also being prescribed to men on testosterone replacement therapy (TRT) as a way to keep estrogen levels from increasing when exogenous testosterone is introduced.
A small, controlled study demonstrated that anastrozole in a dose of 1 mg daily during 12 weeks will result in doubling of the mean bioavailable testosterone level in older men. Aromatase inhibitors are also being prescribed to men on testosterone replacement therapy (TRT) as a way to keep estrogen levels from increasing when exogenous testosterone is introduced.
This is the study that made so many people rave about Aromasin. And let’s be honest the numbers are gooood!
"Pharmacokinetics and Dose Finding of a Potent Aromatase Inhibitor, Aromasin (Exemestane), in Young Males"
Suppression of estrogen, via estrogen receptor or aromatase blockade, is being investigated in the treatment of different conditions. Exemestane (Aromasin) is a potent and selective irreversible aromatase inhibitor. To characterize its suppression of estrogen and its pharmacokinetic properties in young healthy males. In a cross-over study, 12 were randomly assigned to 25 and 50 mg exemestane daily, orally, for 10 days with a 14-day washout period. Blood was withdrawn before and 24 hour after the last dose of each treatment period.
These are the results of the first detailed study of the pharmacological effects of exemestane in male subjects. Doses of 25 and 50 mg were comparable in suppressing all circulating estrogens and had similar effects of increasing serum androstenedione and testosterone concentrations. There were mean 38%, 71%, and 45% decreases in estradiol, estrone, and estrone sulfate concentrations, respectively, after 10 days, approximately 24 hours after administration of the last dose of 25 mg exemestane, coupled with 60% increases in testosterone and 32% increases in androstenedione concentrations. The rise in the aromatase substrates, testosterone and androstenedione, is probably secondary to substrate accumulation and/or to the feedback increase in gonadotropins caused by aromatase blockade.
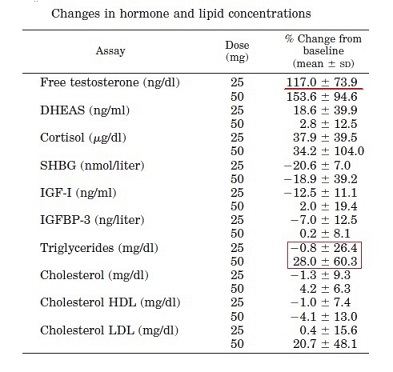
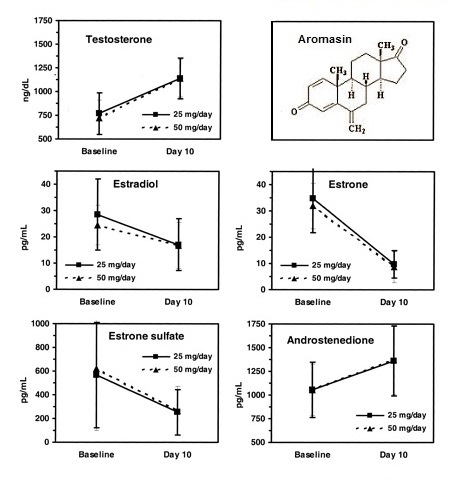 SHBG concentrations were decreased by a mean 21% and 19% at 25 and 50 mg exemestane, respectively.
SHBG concentrations were decreased by a mean 21% and 19% at 25 and 50 mg exemestane, respectively.
At the end of the 10 days, total testosterone had increased ~60% but free testosterone (that is, the testosterone that is actually free to bind the androgen receptor ) increased by 117%.
The reason this works is because estrogen is reduced as a result of the aromatase blockage, and estrogen is the main negative feedback signal to the hypothalamus to decrease LH secretion. So with lower estrogen in the system, more LH is secreted and more testosterone is made. It’s a double whammy as well, because with aromatase blockage, less testosterone is lost in the conversion to estrogen.
In fact another recent report even suggested aromatase inhibitors may be of benefit to obese men who suffer from hypogonadism due to the excess estrogen that usually accompanies obesity. And of course “natural bodybuilders”, anecdotically the combination bodybuilding/fitness/lifting combined with Aromasin works!!
Whether or not this increased testosterone will result in anabolic affects however is up for debate. However if you think your suffering from low testosterone, aromasin could be of some help. Aromasin is actually quite a safe drug, with minimal side effects, but it is slightly pricey.
Note in the first study, estrogen levels returned to normal 3-6 days after aromasin withdrawal, so the drug must be continuously taken to keep the increased levels of testosterone.
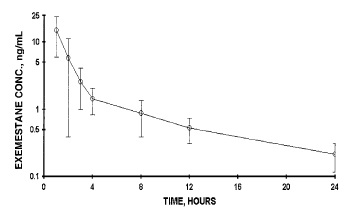 The terminal half-life in the present study (~9 hours) was considerably shorter than the published value of 27 hours (in postmenopausal women). The reason for this difference is not clear, but may be related to a true gender dependency possibly involving the volume of distribution (lower in males than females) and plasma or tissue protein binding (respectively, higher and lower in males).
The terminal half-life in the present study (~9 hours) was considerably shorter than the published value of 27 hours (in postmenopausal women). The reason for this difference is not clear, but may be related to a true gender dependency possibly involving the volume of distribution (lower in males than females) and plasma or tissue protein binding (respectively, higher and lower in males).
The maximal suppression evoked by exemestane at the single dose of 25 mg in the present study was similar to published results in postmenopausal women, but the time course differed. Evans et al. (reported that a single 25-mg oral dose of exemestane maximally suppressed estradiol concentrations by 72% 3 d after administration, and estradiol levels returned to baseline only 8–11 d after drug administration.
 Graph: Percent change from baseline in plasma estradiol concentrations after a single 25-mg dose of exemestane in 10 young men.
Graph: Percent change from baseline in plasma estradiol concentrations after a single 25-mg dose of exemestane in 10 young men.
In the present study maximal suppression of estradiol of 62% was observed 12 hours after exemestane administration and returned to baseline 3–6 d after administration.
The reason for this difference is not clear, but may be related to the shorter half-life of exemestane in males, the lower exposure to exemestane, and the higher levels of the aromatase substrates androstenedione (1 ng/ml in young males vs. 0.5 ng/ml in postmenopausal women), particularly the much higher testosterone concentrations in young males than in postmenopausal women (700 ng/dl vs. 20 ng/dl, respectively) (25). This is supported by the observation that in the 10-d study in young males reported here, the suppression of estradiol is weaker (due to the very high levels of the precursor testosterone) than that of estrone (due to androstenedione levels not very different from those in postmenopausal women).
A limited suppression of circulating estradiol (50%) has been reported in a similar study in young males treated with 1 mg daily anastrozole (ARIMIDEX), a dose that reduces estradiol by 85% in postmenopausal women!!
Dosing
 Dosing is individual, that is true for roids and also for anti-e or aromatase inhibitors. It also depends on other variables like gender, cycle, cycle length, height/weight etc. On light cycles 12.5mg Aromasin twice a week or 0.25mg Arimidex twice a week should be enough to regulate estrogen levels while increasing overall testosterone.
Dosing is individual, that is true for roids and also for anti-e or aromatase inhibitors. It also depends on other variables like gender, cycle, cycle length, height/weight etc. On light cycles 12.5mg Aromasin twice a week or 0.25mg Arimidex twice a week should be enough to regulate estrogen levels while increasing overall testosterone.
Just look at the numbers in this blogpost and then decide. Like I said if you do use, take what you need and not too much. Some do 6.25 mg every day (ed) or 12 mg every other day (eod). Some even do 12.5 mg (half tablet) every 4th day (e4d). I would advise to use it with Nolvadex. Most guys will advise a tablet per day. If you use not enough you will bloat and/or lose your libido. If you use to much you will suffer stiff joints. Many guys will tell you if you are using the right amount you will experience a feeling of well being.
Conclusion:
Suddenly everyone is convinced about Aromasin and wants to use it. But..maybe it’s better to first find out if this compound is really needed for your purposes. Maybe you can do without any anti-E’s or AI’s . Still it’s good to have them available, just in case. I.m.h.o. it is best to use anti’s only when needed. And the old known means are often as good and cheaper and better available. When hardcore with polypharmacy and a few grams gear, products like Aromasin and Arimidex are a gift from heaven.