
distended bellies

Distended bellies also known as GH-gut or roid-gut
The GH gut is well known phenomenon among “modern” bodybuilders. It is widely discussed on bodybuilding-boards, magazines and in the gym. We’ll try to explain the reason why it happened and if there is a way back.
Let us start at the beginning.
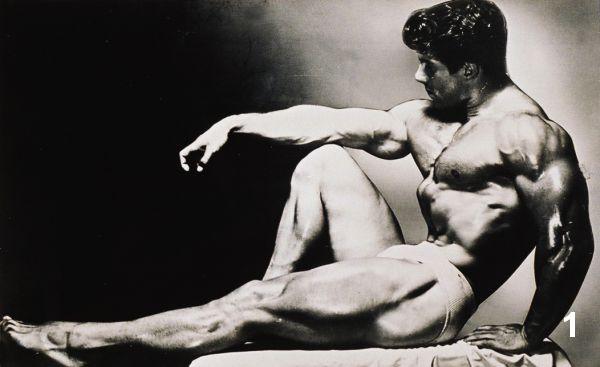
During the Golden Age ( the 1940s and 50s) the champions like Steve Reeves, John Grimek and Reg Park (picture 1) wanted to sculpt their bodies like the statues of the ancient Greek and Roman gods. Their goal was to attain an athletic body with aesthetical size and symmetry. These champions of the pre-steroid time were proud of their health and strength and looks.
 Bodybuilders of the 1960s, had these men as their example, these where athletes such as Arnold Schwarzenegger, Franco Columbo, Bob Paris and Frank Zane. These bodybuilders where the ones that started to use anabolic androgenic steroids, starting with Dianabol (methandrostenolone) small blue pils they called “the breakfast of the champions”.
Bodybuilders of the 1960s, had these men as their example, these where athletes such as Arnold Schwarzenegger, Franco Columbo, Bob Paris and Frank Zane. These bodybuilders where the ones that started to use anabolic androgenic steroids, starting with Dianabol (methandrostenolone) small blue pils they called “the breakfast of the champions”.
These bodybuilders tried hard to achieve a dramatic V-shape, broad shoulders and a narrow waist. This was also shown on stage with the vacume pose. If we compare the Body Mass Index (BMI) of the proffesional bodybuilders from the different ereas, it goes from 28.3 (Steve Reeves), 26.1 (Jack La Lanne) in the 1950s to a mean value of 30 points in the 1980s. In the 1990s when the peptides entered the sport the mean BMI value rose to 35 points in the beginning of 2000 to pro-bodybuilders with a BMI value of 40 or more points in 2006-2007s
Our most popular bodybuilder Arnold Schwarzenegger is 6' 2" (188 mtr) and his competition weight was 235 lbs (107 kg) with a waist of 34". His waist-to-height ratio was 0.46 and his BMI was 30.2. In 1969 he won the Mr. Universe title and he dominated the Mr. Olympia competition from 1970 to 1975. You see that we also include the size of his waistline and the waist-to-height ratio a very commen number in those years. Even a massive man like Lou Ferrigno who won his first Mr. Universe title in 1973 only 21 years of age, had a 34" waist with a bodylength of 6'5" (196 mtr), he weighed 285 pounds (129 kg) and had a waist-to-height ratio of 0.44 and a BMI of 33.9.
 Some bodybuilders with a genetical very small waist like by example Sergio"The Myth" Oliva, had an advantage. Oliva had a 29 inch waist that give him an impressing V-shape.
Some bodybuilders with a genetical very small waist like by example Sergio"The Myth" Oliva, had an advantage. Oliva had a 29 inch waist that give him an impressing V-shape.
Sergio Oliva, who won Mr. Olympia competition in 1967 to 1969 virtually compared to Ronni Coleman, who won the Mr. Olympia contest from 1998 to 2005, makes the difference in bodyshape clearly visible (picture 2).
Ronnie is 5'11" (1.80 mtr) tall and has a competition weight of 296 pounds (134 kg) and has a BMI of 41.4.
Sergio is also is 5'11" (1.80 mtr) tall and has a competition weight of 240lbs (109 kg ) and a BMI of 34.
At the end of the 1990s, beginning years 2000 it was obvious that bodybuilding had created a problem. In the line-up appeared professional bodybuilders with a gross distended waistline. When posing in contest shape it was not that obvious but when they relaxed the muscels some looked like pregnant whales. It was far from eastethic. In their quest to more musclemass the result bad looking topcompetitors. The bodybuilding contest had become freakshows.
On the net people where divided, some of the respondands found that a bigger mass was what bodybuilding was about, while others found that the more easthetic classical physique should win. They blamed the freaky look on the bodybuilding organisations that instructed the judges who classified these look as the winnars physique. Bodybuilding is subjective just like a beautycontest. Everyone has a different opinion and prefers a certain phenotype. In our sport the winnar is mostly attached to a certain organisation and a certain “nutritionist “, these bodybuilders get the pricemoney and the most coverage abd frontpages in the magazines mostly owned by the same group of people.But body building was no longer a healthy clean sport. When the first the first nudepics of the female topcompetitors where posted on the internet even the IFBB understood that they where to far off,
At the end of the 1990s, beginning years 2000 it was obvious that bodybuilding had created a problem. In the line-up appeared professional bodybuilders with a gross distended waistline. When posing in contest shape it was not that obvious but when they relaxed the muscels some looked like pregnant whales. It was far from eastethic. In their quest to more musclemass the result bad looking topcompetitors. The bodybuilding contest had become freakshows.
On the net people where divided, some of the respondants found that a bigger mass was what bodybuilding was about, while others found that the more easthetic classical physique should win. They blamed the freaky look on the bodybuilding organisations that instructed the judges who classified these look as the winnars physique. Bodybuilding is subjective just like a beautycontest. Everyone has a different opinion and prefers a certain phenotype. In our sport the winnar is mostly attached to a certain organisation and a certain “nutritionist “, these bodybuilders get the pricemoney and the most coverage and frontpages in the magazines, mostly owned by the same group of people. But body building was no longer a healthy clean sport. When the first the first nudepics of the female topcompetitors wher on the internet even the IFBB understood that they where to far off.
Before that founder Joe Weider said in an interview: “From the very start, I wanted bodybuilding to be seen not just as a way to build massive muscles, but also as a way to get healthy. I'm afraid that message got lost, and I still want to get it out there”.
The IFBB Pro Division stated in their annual report December 6, 2004: For aesthetics and health reasons, the IFBB Professional Division requests that female athletes in Bodybuilding, Fitness and Figure decrease the amount of muscularity by a factor of 20%.
A year later in the IFBB Pro Division annual report 2005:
With a mandate from President Ben Weider, the Professional Committee and a team of expert advisors recently evaluated the issues associated with muscular development, such as size, shape, density, separation and definition, in relation to symmetry and natural aesthetics.
Certain objective criteria are involved in assessing symmetry and natural aesthetics in competitive bodybuilding. Of great significance are the qualities of balance, proportion and the overall “flow” of the physique, including classic attributes such as a dramatic “V-taper”; from broad shoulders and a wide back to a streamlined waist and a flat, muscular abdomen. In addition, there should be balance between upper and lower body development, and harmony between the left and right sides of the body. These characteristics have been the hallmark of a bodybuilder’s physique for decades, and it is the intent of this Advisory Notice to reaffirm their significance.
Distended abdomens and distorted muscles negatively impact upon symmetry and natural aesthetics and, therefore, detract from the overall physique. Athletes and judges are advised that muscle size at the expense of symmetry and natural aesthetics will not be assessed favourably.
But the genie was out of the bottle, the over sculpted physiques kept the first places in the most important contests. Maybe also the public was to blame they where the people to came to see the contests, bought the magazines and the paraphernalia such as shirts. We see that more and more athletes suffer from health problems. In fact bodybuilding was meant as role model where young bodybuilders could identify themselves with a certain champion and tried to achieve his looks. That surely is no longer advisable. In the off-season some of the top professional bodybuilders look very fat with overextended bellies and a extreme butt. Seen from the side and on YouTube work-out movie-clips they look far from aesthetic.
Before (prenatal) and after (postnatal) birth the body has an high level of growth factors. The child sleeps, eats and is growing . This growing evolves all tissues in the body including bones, hairs, organs and nails. During puberty when the sex hormones come into play the growth stops. The individu no longer attains height, because the growth plates (epiphyseal plates) at the end of the long bones in the arms and legs close. The skeletal frame is now fixed. It is still possible to “mature” and gain some fat and muscles. The ribcage is also flexible because of cartilage bone tissue.
 On the discussion forums and in the magazines it seems It seems that everybody has an other explanation for the exact cause of the distended belly . Some blame the growth hormone, others the insulin. Even the high amount of carbohydrates used in conjunction with the insulin and the off-season bulk period are blamed. Or some even think that the size of the waistline is largely down to genetics. Some people blame the diet too high in carbohydrates, and others say too bulky on off-season.
On the discussion forums and in the magazines it seems It seems that everybody has an other explanation for the exact cause of the distended belly . Some blame the growth hormone, others the insulin. Even the high amount of carbohydrates used in conjunction with the insulin and the off-season bulk period are blamed. Or some even think that the size of the waistline is largely down to genetics. Some people blame the diet too high in carbohydrates, and others say too bulky on off-season.
Far most respondents, writers in magazines and on the net truly believe that recombinant human growth hormone causes the entire body to grow, not only the muscle. So when growth hormone is abused, even the internal organs (visceral organs) grow, causing the distended belly. Hence the name “gh-gut” It is also said that growth hormone causes more internal fat, not subcutaneous (under the skin) , but visceral fat (surrounding the organs).
Most people think its sad how cheap recombinant human growth hormone has transferred bodybuilders from athletic, symmetrical athletes into big cartoon alike mass monsters.
Lets find some scientific explanation for this phenomenon.
Most of the action of growth hormone are mediated through the insulin-like growth factor-1 (IGF-1). Administration of growth hormone induces a rise in circulating IGF-1 (9 )
Very interesting in this regard is a study (12) of artificially feeding-induced intestinal atrophy in combination with exogenous IGF-I, which induces intestinal growth, and exogenous GH, which does not stimulate intestinal growth, to gain insight into the role of IGF-I and insulin receptor binding responses in the regulation of intestinal growth (10, 22) it was the first to use this model.
This already shows us that IGF-1 is in fact responsible for the growth of the intestinal tract. It becomes even more exciting with other scientific researches
Animal studies demonstrating intestinal growth with administration of insulin-like growth factor-I (IGF-I) and insulin strongly support the notion that growth factors, such as IGF-I, GH (GH) and insulin, act on the gastrointestinal tract in an endocrine manner to help mediate nutrient regulated growth . Specific binding sites for IGF-I, GH, and insulin are present in the small and large intestine and evidence suggests that circulating IGF-I, GH, and insulin can interact with their respective functional intestinal receptors. For example, Zeigler et al. demonstrated that rat jejunal IGF-I and insulin receptors are differentially regulated by fasting and refeeding (dieting and bulking). The jejunum is the middle section of the small intestine.
Total parenteral nutrition (TPN) results in marked atrophy of the small intestine in the rat and mucosal hypoplasia in healthy subjects maintained with TPN. We have demonstrated that treatment with rhIGF-I or rhGH produce equivalent, significant increases in circulating levels of IGF-I and body weight gain, and that IGF-I and GH differentially increase protein synthesis in jejunal mucosa and skeletal muscle, respectively . Interestingly, only IGF-I, and not GH, stimulates intestinal growth in parenterally fed rats and orally fed rats subjected to massive intestinal resection . In addition, GH does not stimulate crypt cell proliferation in transgenic mice that over express GH and show increased circulating levels of IGF-I .
The resistance of the small bowel to GH could be due to alterations in IGF-I or insulin receptor binding or postreceptor signaling. Insulin could directly affect mucosal cell proliferation or indirectly modulate IGF-I action. To better understand the selective ability of IGF-I, but not GH, to stimulate intestinal growth, we have compared IGF-I and insulin receptor binding and expression in jejunal membranes from orally fed rats and parenterally fed rats treated with IGF-I, GH or IGF-I plus GH.
Parenteral nutrition and treatment for 3 days with either rhIGF-I or rhGH produced a similar 10 g increase in body weight and animals treated simultaneously with IGF-I and GH showed a significant 15 g increase in body weight compared with total parenteral nutrition (TPN) alone,
This study provides new information about the role of IGF-I and insulin receptors in the regulatory actions of luminal and circulating nutrients, as well as exogenous IGF-I and GH, in mediating small bowel growth. The role of the insulin receptor in stimulation of jejunal growth is unclear. We cannot rule out the possibility that IGF-I action is being signaled in part through the insulin receptor. Given the clinical interest in utilization of IGF-I and GH to promote anabolism in critically ill patients who often require TPN , the current study provides relevant insights into the mechanisms of action of IGF-I and GH in the small bowel.
1. Taylor RG et al, 1994 Humoral regulation of intestinal adaptation. Clin Endocrinol Metab 8:165–183
2. Steeb Cbet al, 1994 Prolonged administration of IGF peptides enhances growth of gastrointestinal tissues in normal rats. Am J Physiol 266:G1090–G1098
3. Peterson CA et al, 1996 Beneficial effects of insulin-like growth factor-I on epithelial structure and function in parenterally-fed rat jejunum. Gastroenterology 111:1501–1508
4. Menard D et al, 1993 Stimulatory effect of insulin on DNA synthesis in suckling mouse colon. Biol Neonate 63:310–315
5. Ryan J et al, 1993 Determination of the histological distribution of insulin-like growth factor I receptors in the rat gut. Gut 34:1693–1697
6. Gingerich RL et al, 1987 Identification and characterization of insulin receptors in basolateral membranes of dog intestinal mucosa. Diabetes 36:1124–1129
7. Lobie, PE et al, 1990 Growth hormone receptor expression in the rat gastrointestinal tract. Endocrinology 126:299–306
8. Zeigler TR et al, 1995 A comparison of rat small intestinal insulin and insulin-like growth factor I receptors during fasting and refeeding. Endocrinology 136:5148–5154
9. T. D. Kimbroughet al. 1991 Insulin-like growth factor-I response is comparable following intravenous and subcutaneous administration of growth hormone, Journal of Surgical Research, vol. 51, no. 6, pp. 472–476
10. Peterson CA et al, 1997 GH elevates serum IGF-I levels but does not alter mucosal atrophy in parenterally-fed rats. Am J Physiol 272:G1100–G1108
11. Yang H et al, 1997 Stimulation of intestinal growth is associated with increased insulin-like growth factor-binding protein-5 mRNA in the jejunal mucosa of insulin-like growth factor-I treated parenterally fed rats. Proc Soc Exp Biol Med 216:438–445
12. D. M. Ney et al, 1999 Investigation of Insulin-Like Growth Factor (IGF)-I and Insulin Receptor Binding and Expression in Jejunum of Parenterally Fed Rats Treated with IGF-I or Growth Hormone. Endocrinology Vol. 140, No. 10 4850-4860
This article is not complete and will be updated. ronny..
- Login to post comments