Creatine

 Creatine is a molecular battery. Cells stick energy-providing phosphate groups on to creatine molecules, and pull them off again when they need them. That’s why power athletes can manage longer sets if they take creatine. The human body gets creatine from foods such as fish and meat, but also makes the substance itself from the amino acids arginine and glycine. When producing creatine, the body also uses methyl groups from the S-adenosylmethionine molecule, which as a result change into homocysteine. Seventy percent of the homocysteine in your body is produced as a result of your body manufacturing creatine. A single 5g dose corresponds to the creatine content of 1.1 kg of fresh, uncooked steak.
Creatine is a molecular battery. Cells stick energy-providing phosphate groups on to creatine molecules, and pull them off again when they need them. That’s why power athletes can manage longer sets if they take creatine. The human body gets creatine from foods such as fish and meat, but also makes the substance itself from the amino acids arginine and glycine. When producing creatine, the body also uses methyl groups from the S-adenosylmethionine molecule, which as a result change into homocysteine. Seventy percent of the homocysteine in your body is produced as a result of your body manufacturing creatine. A single 5g dose corresponds to the creatine content of 1.1 kg of fresh, uncooked steak.
 Creatine has become one of the most popular dietary supplements in the sports nutrition market. The form of creatine that has been most extensively studied and commonly used in dietary supplements is creatine monohydrate (CM). Studies have consistently indicated that CM supplementation increases muscle creatine and phosphocreatine concentrations by approximately 15–40%, enhances anaerobic exercise capacity, and increases training volume leading to greater gains in strength, power, and muscle mass. A number of potential therapeutic benefits have also been suggested in various clinical populations.
Creatine has become one of the most popular dietary supplements in the sports nutrition market. The form of creatine that has been most extensively studied and commonly used in dietary supplements is creatine monohydrate (CM). Studies have consistently indicated that CM supplementation increases muscle creatine and phosphocreatine concentrations by approximately 15–40%, enhances anaerobic exercise capacity, and increases training volume leading to greater gains in strength, power, and muscle mass. A number of potential therapeutic benefits have also been suggested in various clinical populations.
Creatine supplementation is widespread in athletics, and report s indicate that many athletes ingest creatine over long periods of. Surveys indicate that 17-74% of athletes of various ages and sport disciplines use creatine and that as many as 50% of the senior-class members of American high-school football teams use it. 17% of High School Student-Athletes, 30% of the High School Football Players, 28-41% of the NCAA Athletes, 29-57% of the Military and Civilian Health-Club Members, 45-74% of the athletes in Power Sports. And most of the NCAA football and Baseball players. Not to mention fitnessers and bodybuilders, males and females. And most of the fitnessers/bodybuilders that take anabolic steroids uses creatine monohydrate while cycling the drugs and in/or after PCT. The evidence that creatine amplifies the potency of the cycle is of course anecdotal, because no ethical commission would agree with such a study. Still bodybuilders know for a long time that eating lots of (raw) meat enhances their cycles. Just as they consume large amounts of proteins.
s indicate that many athletes ingest creatine over long periods of. Surveys indicate that 17-74% of athletes of various ages and sport disciplines use creatine and that as many as 50% of the senior-class members of American high-school football teams use it. 17% of High School Student-Athletes, 30% of the High School Football Players, 28-41% of the NCAA Athletes, 29-57% of the Military and Civilian Health-Club Members, 45-74% of the athletes in Power Sports. And most of the NCAA football and Baseball players. Not to mention fitnessers and bodybuilders, males and females. And most of the fitnessers/bodybuilders that take anabolic steroids uses creatine monohydrate while cycling the drugs and in/or after PCT. The evidence that creatine amplifies the potency of the cycle is of course anecdotal, because no ethical commission would agree with such a study. Still bodybuilders know for a long time that eating lots of (raw) meat enhances their cycles. Just as they consume large amounts of proteins.
Deldicque et al [2008] found a 250%, 45% and 70% increase for collagen mRNA, glucose transporter 4 (GLUT4) and Myosin heavy chain IIA, respectively after 5 days creatine loading protocol (21 g/d). The authors speculated that creatine in addition to a single bout of resistance training can favor an anabolic environment by inducing changes in gene expression after only 5 days of supplementation. If this protocol would be combined with injectable and oral steroids and maybe some growth factors and increased insulin through injection or by taking the creatine with a lot of simple carbohydrates (sugars). OMG!! Remember this last piece of text is just my imagination ..lol.. and maybe yours.. more seriously:
Studies have indicated that CM is not degraded during normal digestion and that nearly 99% of orally ingested CM is either taken up by muscle or excreted in urine. Further, no medically significant side effects have been reported in literature. Nevertheless, supplement manufacturers have continually introduced newer forms of creatine into the marketplace. These newer forms have been purported to have better physical and chemical properties, bioavailability, efficacy, and/or safety profiles than CM. However, there is little to no evidence that any of the newer forms of creatine are more effective and/or safer than CM whether ingested alone and/or in combination with other nutrients. In addition, whereas the safety, efficacy, and regulatory status of CM is clearly defined in almost all global markets; the safety, efficacy, and regulatory status of other forms of creatine present in today’s marketplace as a dietary or food supplement is less clear.
Creatine is a myostatin blocker
In 2010 a group of researchers did a trial with 27 healthy young (± 24 years) male students. Of these, 8 did nothing – the control group (CON).
The other 19 students trained for 8 weeks using weights. The students went to the gym three times a week, where they did 6 basic exercises that covered all the major muscle groups: bench-press, lat-pulldown, biceps curl, leg press, knee extension and leg curl. The students trained at 60-70 percent of their 1RM, and did three sets of each exercise. The students rested for no longer than 2 minutes between sets.
 Half of the students who trained took creatine (resistance training+creatine RT+CR). The other half who trained took a placebo (resistance training+placebo RT+PL). In the first week they took a daily 0.3 g creatine per kilo bodyweight, and in the remaining weeks they took a daily 0.05 g creatine per kilogram bodyweight. It doesn’t take a genius to work out that the test subjects who trained became more muscular and stronger, and that the creatine supplementation enhanced the effect.
Half of the students who trained took creatine (resistance training+creatine RT+CR). The other half who trained took a placebo (resistance training+placebo RT+PL). In the first week they took a daily 0.3 g creatine per kilo bodyweight, and in the remaining weeks they took a daily 0.05 g creatine per kilogram bodyweight. It doesn’t take a genius to work out that the test subjects who trained became more muscular and stronger, and that the creatine supplementation enhanced the effect.
The researchers measured the concentration of myostatin in the subjects' blood. Weight training reduced the concentration. And training while using creatine reduced the concentration even further.
The researchers measured the concentration of the protein growth and differentiation factor-associated serum protein-1 [GASP-1]. This protein neutralises myostatin.
The production of GASP-1 increased as a result of strength training and it increased even more in the subjects who combined strength training and creatine supplementation.
 The researchers conclude that creatine doesn't just pump up the muscles temporarily. So creatine is a real anabolic, responsible for increased muscle protein production. "Decreasing myostatin and inhibiting its function by GASP-1 may play an important role in increasing muscle strength and mass by resistance training", they write. "Supplementation with creatine resulted in greater increases in muscle mass and strength, and these improvements were accompanied by more decreased myostatin levels."
The researchers conclude that creatine doesn't just pump up the muscles temporarily. So creatine is a real anabolic, responsible for increased muscle protein production. "Decreasing myostatin and inhibiting its function by GASP-1 may play an important role in increasing muscle strength and mass by resistance training", they write. "Supplementation with creatine resulted in greater increases in muscle mass and strength, and these improvements were accompanied by more decreased myostatin levels."
Creatine users manufacture more IGF-1 in muscle tissue
Canadian sports scientists in 2008 studied forty healthy people, males and females in their twenties, that performed resistance weight training, they gave half of them creatine supplements. The other half were given a placebo.
After eight weeks the researchers measured the amount of IGF-1 in the muscles of the subjects. In the placebo group they recorded an increase of 54 percent. In the creatine group the increase was 78 percent.
 IGF-1 has a strong anabolic effect. In athletes the type of IGF-1 that the muscle cells manufacture themselves is important, and this is influenced by training, amino acids and, as we know now, creatine.
IGF-1 has a strong anabolic effect. In athletes the type of IGF-1 that the muscle cells manufacture themselves is important, and this is influenced by training, amino acids and, as we know now, creatine.
In 2005 researchers from Louvain, Belgium reported that they had also found an increased level of IGF-1 in the muscle tissue of human weight trainers.
The Belgians got their subjects to do weight training and gave them a daily dose of 21 g of creatine for five days.
Before each training session the subjects drank a protein shake with carbohydrates.
The effect is clear. Three hours after training, when your muscles start to recover and hopefully grow, the production of IGF-1 increases more if you use creatine.
The Belgians also demonstrate in their article that creatine makes other anabolic signaling molecules in muscle cells more active, such as 4E-BP1 and p70-S6K. This leads them to conclude that "creatine supplementation could act to stimulate muscle growth, but not by a rapidly responding control system as observed after exercise plus feeding, but rather by a late-response enhancement of the anabolic status of the cell involving IGF".
So one could say creatine is not only a training booster, but an anabolic agent as well.
Creatine users have more DHT in their blood
Creatine may increase muscle mass and strength through an additional mechanism and not just by increasing the amount of energy-generating phosphate groups in the muscles. According to sports scientists at Stellenbosch University, South Africa, creatine increases the amount of the androgenic testosterone metabolite DHT. in the muscles.
 In an article in the Clinical Journal of Sport Medicine, the South Africans describe an experiment they did with twenty rugby players, average age 19. Half of them took a placebo for three weeks. The other half were given creatine and glucose. The function of the glucose was to improve the uptake of creatine in the muscle cells.
In an article in the Clinical Journal of Sport Medicine, the South Africans describe an experiment they did with twenty rugby players, average age 19. Half of them took a placebo for three weeks. The other half were given creatine and glucose. The function of the glucose was to improve the uptake of creatine in the muscle cells.
The test subjects in the experimental group took a daily dose of 25 g creatine and 25 g glucose for the first week. In weeks 2 and 3 they took a daily 5 g creatine and 25 g glucose.
The bodies of the test subjects in the experimental group reacted to the creatine in the way you'd expect the bodies of serious athletes for whom weight training is not the core fitness activity to react. Their lean body mass increased slightly and their fat percentage decreased by a miniscule amount.
 Nothing new so far. But when the researchers did a blood analysis of the hormone levels in the players, they made a discovery. At the end of the first week, during which the rugby players had taken 25 g of creatine a day, their DHT level had risen by 56 percent. In the following weeks, when they took a lower creatine dose, the subjects' DHT level went down, but remained raised. This effect was a large increase in DHT rather than a marginal and possibly physiologically insignificant effect.
Nothing new so far. But when the researchers did a blood analysis of the hormone levels in the players, they made a discovery. At the end of the first week, during which the rugby players had taken 25 g of creatine a day, their DHT level had risen by 56 percent. In the following weeks, when they took a lower creatine dose, the subjects' DHT level went down, but remained raised. This effect was a large increase in DHT rather than a marginal and possibly physiologically insignificant effect.
The testosterone concentration in the test subjects' blood remained constant. You'd expect the test subjects would also have produced less estradiol, but the South Africans don't mention estradiol at all in their article.
The researchers suspect that a creatine supplement increases the activity of the enzyme 5-alpha-reductase somewhere in the body. This enzyme converts testosterone into DHT, but exactly where this takes place the researchers don't know. Not in the muscles is all they can say for sure, as the muscles don't contain much 5-alpha-reductase.
Nor are the researchers sure whether the athletes build up more muscle fie as a result of the metabolic change. This could be the case, they speculate: "Biochemical studies of androgen receptor affinity indicate that DHT is 4 times more biologically potent than testosterone". The buildup of muscle in creatine users, so often reported by sports scientists, may be partly due to endocrinal changes.
The scientists believe that their discovery is important for athletes. They warn of the potential side-effects of creatine, and argue that more research should be done on whether creatine increases the risk of baldness and benign enlargement of the prostate.
Caffeine and Creatine
 Caffeine has been shown to enhance endurance exercise performance even at doses well below the reference limit. Although some researchers claim that caffeine has no effect on short and intense exercise, a large number of studies have shown significant improvements in power output and anaerobic performance.
Caffeine has been shown to enhance endurance exercise performance even at doses well below the reference limit. Although some researchers claim that caffeine has no effect on short and intense exercise, a large number of studies have shown significant improvements in power output and anaerobic performance.
Ok, so it has been shown that caffeine probably benefits in exercise but what about when you combine it with creatine, which is often the case? Caffeine consumption has been reported to adversely affect the efficacy of creatine supplementation. Vandenberghe et al. concluded that the ergogenic effect of creatine is completely eliminated by caffeine consumption. Torque was increased by up to 23% in creatine group while it was unchanged in the creatine + caffeine group. In a follow-up study, same researchers reported that caffeine consumption inhibits phosphocreatine resynthesis during recovery .
One of the more recent studies indicated that a single dose of caffeine following short-term creatine supplementation did not hinder the creatine–caffeine interaction. It actually lengthened time to exhaustion.
It appears that caffeine at least partially negates the effect of creatine. However, caffeine does not negate the benefits of creatine loading when not coingested. It may be a good strategy to load creatine without caffeine and save caffeine for selected workouts as it enhances creatine’s effectiveness in anaerobic exertion if the two compounds are alternated.
 Creatine on hypertrophy
Creatine on hypertrophy
A study of Young et all 2007, investigated the effect of dietary creatine supplementation on hypertrophy and performance of rat skeletal muscle. Male Sprague-Dawley rats underwent either tibialis anterior ablation or partial ablation of the plantaris/gastrocnemius to induce compensatory hypertrophy of the extensor digitorum longus (EDL) or soleus respectively, or sham surgery. Creatine (300 mg/kg) was administered to one half of each group for 5 weeks, after which force production was measured. With the leg fixed at the knee and ankle, the distal tendon of the EDL or soleus was attached to a force transducer and the muscle was electrically stimulated via the sciatic nerve. Synergist ablation resulted in a significant increase in EDL mass and in soleus mass relative to control muscles. However, no effect of creatine supplementation on muscle mass or performance was found between control and either group of creatine-treated rats. Despite an apparent increase in muscle creatine content, creatine supplementation did not augment muscle hypertrophy or force production in rat EDL or soleus muscle, providing evidence that the potential benefits of creatine supplementation are not due to a direct effect on muscle but rather to an enhanced ability to train.
Creatine as an anti-oxidant
People with high amounts of homocysteine in their blood are not healthy and have an increased chance of a heart attack. How this happens is not known. Until recently researchers thought that homocysteine itself was responsible for this, but this theory has been rejected. That extremely high concentrations of homocysteine, such as are found in metabolic disorders or serious anabolic steroid use, do pose considerable risk is not disputed by researchers – ed. In trials, vitamin B supplements did lower the concentration of homocysteine, but did not reduce the risk of a heart attack. Apparently something goes wrong in the body’s homocysteine production process.
And that’s where creatine comes into the equation. consume creatine,and the production of homocysteine goes down.
Animal studies performed by nutritionists from the University of Sao Paulo who did experiments with rats.
 Thirty rats were divided into three groups: control group; diet with creatine group (DCr; 2 % creatine in the diet for 28 d); creatine overload plus diet with creatine group (CrO + D; 5 g creatine/kg by oral administration for 5 d + 2 % in the diet for 23d). Plasma homocysteine (Hcy) was significantly lower in DCr (7·5 (SD 1·2) μmol/l) and CrO + D (7·2 μmol/l) groups compared with the control group (12·4 μmol/l).
Thirty rats were divided into three groups: control group; diet with creatine group (DCr; 2 % creatine in the diet for 28 d); creatine overload plus diet with creatine group (CrO + D; 5 g creatine/kg by oral administration for 5 d + 2 % in the diet for 23d). Plasma homocysteine (Hcy) was significantly lower in DCr (7·5 (SD 1·2) μmol/l) and CrO + D (7·2 μmol/l) groups compared with the control group (12·4 μmol/l).
The creatine supplement reduced the concentration in the blood of TBARS, a marker for free radical damage. The more creatine the rats had in their blood, the lower the TBARS concentration. The concentration of free radicals, such as hydrogen peroxide, was also lower.
What’s more, the lower the TBARS concentration in the rats’  blood, the lower their homocysteine level.
blood, the lower their homocysteine level.
Creatine also reduced the production of the endogenous antioxidant glutathione. Glutathione is a tripeptide that is used by detoxifying enzymes like glutathione S-transferase. The researchers suspect that creatine supplementation results in the body needing less glutathione. They think that creatine itself works as an antioxidant.
Research on creatine and homocysteine is doubly interesting for strength athletes and bodybuilders. Because they have more muscle mass, their body makes more creatine and they have more homocysteine in their body. That’s why the homocysteine level goes down in transsexuals that change from man to woman, and thus give up muscle mass.
Using anabolic steroids raises the concentration of homocysteine even further. In studies from 2006, on juiced bodybuilders, a raised homocysteine level heralded a fatal heart attack.
Creatine absorption
Harris et al wanted to test whether creatine given as a supplement to normal subjects was absorbed, and if continued resulted in an increase in the total creatine pool in muscle. An additional effect of exercise upon uptake into muscle was also investigated.
Low doses (1g of creatine monohydrate or less in water) produced only a modest rise in the plasma creatine concentration, whereas 5g resulted in a mean peak after 1h of 795 (SD 104) mumol/l in three subjects weighing 76-87 kg. Repeated dosing with 5g every 2h sustained the plasma concentration at around 1000 mumol/l. A single 5g dose corresponds to the creatine content of 1.1 kg of fresh, uncooked steak.
Supplementation with 5g of creatine monohydrate, four or six times a day for 2 or more days resulted in a significant increase in the total creatine content of the quadriceps femoris muscle measured in 17 subjects. This was greatest in subjects with a low initial total creatine content and the effect was to raise the content in these subjects closer to the upper limit of the normal range. In some the increase was as much as 50%.
Factors Influencing Muscle Creatine Uptake Following Supplementation
The strongest determinant of how much creatine will be taken up into muscle following supplementation is the initial creatine content in that muscle. 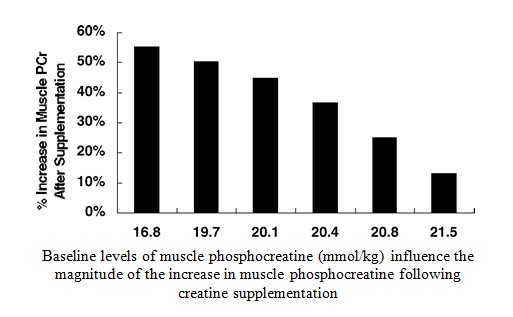
Subjects with lower muscle creatine stores have the greatest increase in muscle creatine following supplementation, whereas subjects with higher creatine levels will experience little or no increase in muscle creatine. However, this cannot fully explain the large intersubject variability in the response.
Uptake into muscle was greatest during the first 2 days of supplementation accounting for 32% of the dose administered in three subjects receiving 6 x 5g of creatine monohydrate/day. In these subjects renal excretion was 40, 61 and 68% of the creatine dose over the first 3 days. Approximately 20% or more of the creatine taken up was measured as phosphocreatine. No changes were apparent in the muscle ATP content.
Creatine and sugars
What is the amount of sugars needed to boost creatine retention during the first week loading phase. Not 25 grams, not 50, but 90+ grams with each dose of creatine. Lower amounts have never been shown to boost creatine retention, and likely do not because they don't produce a big enough insulin "spike."
Newer research has shown that cutting the sugar load by half and replacing it with protein produces the same boosting effect. One can load this way for 1-2 days and get the same (or perhaps greater) muscle creatine retention boost that 5 days of "normal" loading (creatine only) produces. Many forget that protein itself can increase blood insulin-combined with carbs it often is more potent than carbs alone. During "maintenance" (after week 1), an ideal strategy would be to take approximately 5 grams of creatine 1 to 2 times a day with a meal or post-workout meal. To date, no studies have compared the effectiveness of taking 'creatine alone' compared with taking 'creatine with carbs' during "maintenance."
Animal and in vitro research in the 1970s demonstrated that insulin enhanced the transport of creatine from the circulation into the skeletal muscle of rats
(Koszalka et al., 1972; Haugland & Chang, 1975). Subsequently, several clinical studies reported increased muscle creatine uptake or decreased urinary creatine losses during creatine supplementation accompanied by insulin infusions, carbohydrate ingestion, and ingestion of a combination of carbohydrate and protein. For example, Green et al. (1996a, b) showed that ingesting a high dose of carbohydrate (~90 g, 4 times/day) concurrently with creatine can reduce urinary creatine losses and increase muscle creatine accumulation when compared to supplementation with creatine alone. Because, these high doses of carbohydrate may not be practical for all athletes, other investigators examined the effects of lesser amounts of carbohydrate or carbohydrate/protein combinations on muscle creatine uptake. For example, Preen et al. (2003) reported that the ingestion of creatine and 1 g glucose/kg body mass twice daily increased muscle total creatine by 9% more than ingestion of creatine alone, and Steenge et al. (2000) concluded that the ingestion of creatine with ~ 50 g of a carbohydrate-protein combination causes increases in muscle creatine similar to those observed after ingesting creatine with ~ 100 g of carbohydrate.