
Clenbuterol or albuterol


Clenbuterol has been used for years for its ability to shed body fat and preserve lean muscle mass. Although this is highly debated, clenbuterol has been thought to have mild anabolic properties, which is believed to be the reason for the preservation of muscle mass when dieting. Bodybuilders have used clenbuterol as a diet drug for over three decades, and until the last 10 years or so, most of the clenbuterol came from Mexico and Europe.
Since then, China took over as the largest pharmaceutical raw material supplier in the world. Clenbuterol is very very potent, its effective in micrograms. Tablets are mostly dosed as 0.02 or 0.04 mg (milligram). On the above picture you can see how little is needed to produce 10.000 tablets. It’s obvious that it is very hard to dose such a small amount of API powder (active ingredient). That’s why many underground tabs where dosed to low or too strong. And even some pharmaceutical made (?) Chinese tabs made sure bodybuilders in the Netherlands felt the need to rush to the hospital. Mixing APIs potent in micrograms, such as clenbuterol and T3, takes very long and needs to be done in various steps increasing the binders. That’s why it’s better to make sure you purchase REAL pharma grade tabs when you are using such compounds.
Necrosis of the Heart
Older studies that showed myocardial necrosis and apoptosis in rats, used extremely high doses. The amount administered by injection to the rats was dosed in mg/kg. Yes that's milligrams not micrograms (there is a 1000 fold difference between these two).
So let’s say you are an 80Kg person, you would need to take 400mg in order to have the same dose as the rats did per kg. Compare this with the 80mcg that we typically use for weight loss. This is a factor of 5000 times higher than our normal dose. If you would try to take anywhere close to this, I would expect you to suffer a massive heart attack and die, way before any necrosis took hold. Because of these huge doses, many bodybuilders on the boards, took these animal studies not seriously.
Newer studies also include lower (realistic) human dosages. Because of all those warnings based on absurd high doses in rodents and other animals, bodybuilders found the risks exaggerated and just used clen as they were used to.
Now there is a big individual tolerance and there is also a big tolerance difference between humans and rats, but not enough to balance between micrograms and milligrams. Still  many people using clenbuterol for slimming, use way too much, don’t taper up or down or simply overdose. For many people from recreative bodybuilders, housewives, fitnessers to models and celebrities everyone wants to become slimand lean. Just GOOGLE on clenbuterol. And it works, just like with T3 and often the combination T3 – clenbuterol - just google on the before and after pics. But we need to know that it can be damaging, especially in the long term.
many people using clenbuterol for slimming, use way too much, don’t taper up or down or simply overdose. For many people from recreative bodybuilders, housewives, fitnessers to models and celebrities everyone wants to become slimand lean. Just GOOGLE on clenbuterol. And it works, just like with T3 and often the combination T3 – clenbuterol - just google on the before and after pics. But we need to know that it can be damaging, especially in the long term.
In a study from the University of Melbourne, clenbuterol yielded three very negative changes. First, after just four weeks, clenbuterol-treated rats were unable to maintain their normal swimming or running training intensities, while clean rodents were quite capable of continuing. Secondly, the hearts of the clenbuterol-taking, trained rats increased dramatically in size compared to the hearts of sedentary rats, but the heart expansion was probably due to the infiltration of collagen fibres into the heart walls, not an increase in heart-muscle cells. Collagen is a tough connective tissue which doesn't augment heart-muscle power but in fact stiffens the heart, potentially leading to a decrease in cardiac output. Increases in collagen may also produce cardiac arrhythmias. Thirdly, clenbuterol rats suffered from noticeable cardiac-cell degeneration. This study used 2 milligrams per kilogram of body weight per day(!!)
Low Dose Clen Induces Cardiac Apoptosis
It's been known for some time that clenbuterol at high doses causes cardiac necrosis. This study in animals shows that doses of 1 mcg/kg BW induce apoptosis (programmed cell death) in heart tissue. Humans not uncommonly ingest this much clenbuterol. For instance, in a 220 lb (100 kg) bodybuilder this translates to 100 mcg. (Burniston et all 2004)
Dose-dependent apoptotic and necrotic myocyte death induced by the beta2-adrenergic receptor agonist, clenbuterol. Burniston et all 2005
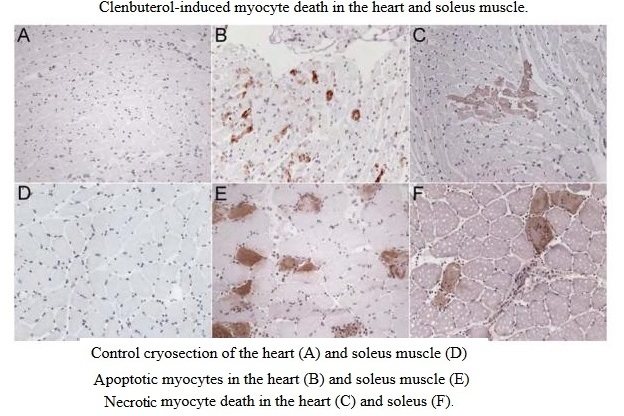
We have investigated the dose- and time-dependency of myocyte apoptosis and necrosis induced by the beta2-adrenergic receptor agonist, clenbuterol, with the aim of determining whether myocyte apoptosis and necrosis are two separate processes or a continuum of events. Male Wistar rats were administered subcutaneous injections of clenbuterol, and immunohistochemistry was used to detect myocyte-specific apoptosis and necrosis. Myocyte apoptosis peaked 4 h after, and necrosis 12 h after, clenbuterol administration. In the soleus, peak apoptosis was induced by 10 mug and peak necrosis by 5 mg x kg(-1) clenbuterol. Twelve hours after clenbuterol administration, 73% of damaged myocytes labeled as necrotic, 27% as apoptotic and necrotic, and 0% as purely apoptotic. Administrations of clenbuterol (10 microg x kg) at 48-h intervals induced cumulative myocyte death over 8 days. These data show that the phenotype of myocyte death is dependent on the magnitude of the insult and the time at which it is investigated. Only very low doses induced apoptosis alone; in most cases apoptotic myocytes lysed and became necrotic and the magnitude of necrosis was greater than that of apoptosis. Thus, it is important to investigate both apoptotic and necrotic myocyte death, contrary to the current trend of only investigating apoptotic cell death.
Case Studies
It’s not only the previous mentioned groups of people interested in getting slim and attractive, also bodybuilders (Andreas Müntzer) sometimes overdose. Just Google and you will find many case studies like this one: “Myocardial infarction in a 17-year-old bodybuilder using clenbuterol”.
CHINA
Livestock growers have learned that clenbuterol can be used to increase muscle to improve the animal’s muscle to fat ratio, producing leaner meats at a much faster rate. Using clenbuterol (and other beta-2 agonists) in animal feed can double profits. 
Left: Sudden death from shòu ròu jīng induced heart failure.
On the way transporting pigs from Henan to Nanjing, a pig died suddenly. The driver says sudden deaths usually happen. The pigs were fed too much shòu ròu jīng and died of heart failure. This dead pig was pulled to the side of the road, and chopped into parts to be sold.
In September of 2006 a large case of food poising involving clenbuterol occurred in Shanghai, China when 336 people were hospitalized after ingesting pig meat that was contaminated with the feed additive. The Chinese government has since taken steps to eliminate clenbuterol from animal feed, which has resulted in clenbuterol to become more restricted and regulated than most other pharmaceutical raw materials in China. With this extreme regulation, albuterol has taken its place with many research companies on the internet.
Since then albuterol has become a popular drug with many bodybuilders trying to lose body fat, there have been many different views when comparing clenbuterol and albuterol. Both drugs are beta-2 adrenoreceptor agonists, which act on the beta-2 adrenergic receptor, causing a dilation of bronchial passages, vasodialation in muscle and liver, and a release of insulin. These characteristics have made this class of drugs a prime choice in treating asthma.
Ketotifen
Both drugs, clenbuterol and albuterol, are often used in conjunction with Ketotifen Fumarate. Ketotifen mostly abbreviated to Keto by bodybuilders, works synergistically with beta-2 adrenoreceptor agonists.
When comparing these two drugs, we must understand how they work, which requires taking a look at the beta-adrenergic system. This system is comprised of adrenoreceptors, but what is relevant here are the beta-receptors. The beta-receptors are located in the cell’s phospholipid membrane, and are stimulated by stimulants like clenbuterol, albuterol, and ephedrine. The beta-receptors can be divided into three subtypes (1,2,3), but when looking at clenbuterol and albuterol, the beta-2 receptor is what we are focusing on. Stimulation of the receptors from stimulants like clenbuterol or albuterol causes a breakdown of fatty acids into the bloodstream to be used as fuel. With this stimulation there will be an increase in heart rate and body temperature.
Beta-2 adrenoreceptor agonists, such as clenbuterol and albuterol, have been shown to activate cyclic-Adenosine Monophosphate (cAMP). cAMP then activates calpistatin, which inhibits calpain. Calpain degrades protein in muscle tissue. By inhibiting calpain, beta-2 adrenoreceptor agonists have been shown to be anti-catabolic. This becomes very beneficial when trying to shed body fat while wanting to preserve muscle mass. A bodybuilder’s goal is always to become as lean as possible while holding as much muscle mass as possible. This is why this class of drugs has always been very popular among this group.
Anabolic properties of beta-2 adrenoreceptor agonists
 You would be better off to use albuterol as opposed to Clenbuterol.
You would be better off to use albuterol as opposed to Clenbuterol.
Clenbuterol has a half-life much longer then Albuterol which makes it more detrimental to heart health. The side effects such as the shaky hands and such are caused from the effects of a specific isomer (S-isomer) included in the medication. Clen is made up of two isomers S and R. R gives you all the respiratory benefits and S gives you the bad effects and reverses the good effects to a certain point. Newer drugs have since been developed that don’t include the S isomer, but these drugs wouldn’t work as well for fat loss as the S isomer aids in thermogenesis. The LD50 of Albuterol (which is the lethal dose in 50% of the population used by pharmacists to judge the potency of a drug) is >2500 mg/kg, the LD50 in Clenbuterol is 80-180 mg / kg the allowable dose 100-140 μg / day in men and 80-100 μg / day in women.
Albuterol can be viewed as a shorter acting version of clenbuterol. They both stimulate the beta-receptors in a similar manner. When looking at beta-2 agonists that are longer acting than clenbuterol, and then compared to clenbuterol, clen had a better rating when it came to anabolic effects. So it would be logical to think that maybe albuterol has an even higher anabolic effect than clenbuterol due to the shorter half-life, but it isn’t always that simple. There is still much more that needs to be studied and looked at before determining this.
The anti-catabolic effects of clenbuterol and albuterol are a plus, but the primary goal of  taking either drug is for fat loss. When honestly looking at things, there are far too many other substances that carry more weight in preserving muscle mass than any beta-2 agonist when there is a deficit in calories. Anabolic steroids and human growth hormone cast a shadow over clenbuterol or albuterol when it comes to preserving lean muscle mass. Most bodybuilders that are dieting are usually taking one or both of these substances, so the anti-catabolic effect is not much of a factor compared to the fat loss that occurs from either of these drugs.
taking either drug is for fat loss. When honestly looking at things, there are far too many other substances that carry more weight in preserving muscle mass than any beta-2 agonist when there is a deficit in calories. Anabolic steroids and human growth hormone cast a shadow over clenbuterol or albuterol when it comes to preserving lean muscle mass. Most bodybuilders that are dieting are usually taking one or both of these substances, so the anti-catabolic effect is not much of a factor compared to the fat loss that occurs from either of these drugs.
 When comparing clenbuterol and albuterol in the category of fat loss, the half-life has to be looked at. Clenbuterol has a (biphasic) half-life of about 48 hours, but in “real life” dosing its said to have a half-life of 7-9 hours, while albuterol has a half-life of just about 3-4 hours. There is an upside and downside to the half-life to both of these drugs. The long half-life associated with clenbuterol will allow a person to dose less often with the drug still staying active in the system and doing its job with burning body-fat. The downside to this long half-life is that the body stops responding to this drug fairly quickly and a possible build-up. This requires a person to cycle the drug 2 weeks on and 2 weeks off, or the person will have to dramatically increase the dose after 2 weeks to feel any effect at all. The short half-life of albuterol requires a person to have to dose more often throughout the day for the drug to be most effective, but tolerance is not built up nearly as fast as it is with clenbuterol.
When comparing clenbuterol and albuterol in the category of fat loss, the half-life has to be looked at. Clenbuterol has a (biphasic) half-life of about 48 hours, but in “real life” dosing its said to have a half-life of 7-9 hours, while albuterol has a half-life of just about 3-4 hours. There is an upside and downside to the half-life to both of these drugs. The long half-life associated with clenbuterol will allow a person to dose less often with the drug still staying active in the system and doing its job with burning body-fat. The downside to this long half-life is that the body stops responding to this drug fairly quickly and a possible build-up. This requires a person to cycle the drug 2 weeks on and 2 weeks off, or the person will have to dramatically increase the dose after 2 weeks to feel any effect at all. The short half-life of albuterol requires a person to have to dose more often throughout the day for the drug to be most effective, but tolerance is not built up nearly as fast as it is with clenbuterol.
Albuterol has a more mild stimulant effect than clenbuterol, and some people find it easier to focus while taking albuterol than clenbuterol. Clen leaves some people shaky, sweaty, and unable to focus during a workout, so albuterol would be the obvious choice. When dieting, some people feel sluggish and find it hard to power though a workout without a strong stimulant. Clenbuterol will often give them that extra edge to push through a workout they normally couldn’t while dieting. Clenbuterol would be the choice for this group.
Effects of oral albuterol on serum lipids
Maki et al in 1996 found in a study that evaluated the effects of a beta(2)-agonist, albuterol, on serum lipids and carbohydrate homeostasis in eight healthy nonsmoking men aged 24 to 61 years:
“Significant alterations were observed in total cholesterol ( -9.1% ), low-density lipoprotein cholesterol ( -15.0%), and high-density lipoprotein cholesterol ( +10.4% ) concentrations, as well as the TC/HDL-C (-17.4% ) and LDL-C/HDL-C (-22.9% ) ratios. During washout, TC and LDL-C returned to baseline levels, whereas HDL-C remained elevated by 5.8% . Thus, albuterol administration was associated with favorable changes in the serum lipid profile without marked impairment of glucose tolerance or its physiologic determinants.
Chazan et al in 1985: “At the end of the second week of oral treatment with salbutamol, the HDL-cholesterol concentration in serum increased by 6.9% .”
Side Effects
Although the manufacturer lists numerous possible side effects, the use of Albuterol and its beta-agonist relatives generally result in very few which typically include: shakiness or slight tremors; increased mental alertness; muscle cramping; difficulty falling asleep and; slightly accelerated (not irregular) heartbeat. (To fight these sides Ketotifen Fumerate is used).
 However, when excessive amounts are taken, or when someone is reacting poorly to these medications they often experience: dizziness; headaches; uncontrollable shaking of a part of the body; nosebleeds; nausea; fast pounding or irregular heartbeat; chest pains; fevers; blisters or rash; hives; swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs; difficulty breathing; difficulty swallowing and hoarseness.
However, when excessive amounts are taken, or when someone is reacting poorly to these medications they often experience: dizziness; headaches; uncontrollable shaking of a part of the body; nosebleeds; nausea; fast pounding or irregular heartbeat; chest pains; fevers; blisters or rash; hives; swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs; difficulty breathing; difficulty swallowing and hoarseness.
Case study
Several reports of clenbuterol overdose are present in the medical literature, including a recent report that demonstrates the immediate risks involved in using the drug.10-13 In this case, a 31-year-old bodybuilder was admitted into the emergency room complaining of heart palpitations (irregular or forceful heartbeat) and shortness of breath; he was also quite anxious.14 Surprisingly, his body temperature was not elevated (97.1º; normal body temperature is 98.6º). The doctors discovered that his heart rate was alarmingly high— 254 beats per minute. The formula for maximum heart rate commonly referenced is 220 minus your age (189 beats per minute in this case), so this person was clearly overly stimulated. In fact, the electrical process involved in heart contractions (remember, the heart is a specialized muscle) has a theoretical limit of 300 beats per minute and this cannot be maintained. This condition, called supraventricular tachycardia, is often seen in stimulant drug overdoses (cocaine, methamphetamine, etc).15,16
 Even after initial drug treatment, the patient’s heart rate remained elevated. A toxicology specialist was called in and further treatment with a beta-blocker (to reverse clenbuterol’s stimulation of the b1-receptors on the heart) managed to lower the heart rate to a safe range. However, as the heart rate dropped into normal range, a second and more dangerous abnormal heart rhythm emerged called atrial fibrillation. Fibrillation is a term that describes a type of shivering motion of the heart muscle that does not pump blood. Instead, the blood pools and quivers. This is dangerous not only because it provides poor circulation, but also because blood will clot if it is not in motion. Atrial fibrillation is one of the main causes of embolic strokes and pulmonary embolism (clots in the lung), both which can be fatal.17 After two days, the condition did not change and the patient was cardioverted (shocked using paddles) to shock the heart back into a normal rhythm.
Even after initial drug treatment, the patient’s heart rate remained elevated. A toxicology specialist was called in and further treatment with a beta-blocker (to reverse clenbuterol’s stimulation of the b1-receptors on the heart) managed to lower the heart rate to a safe range. However, as the heart rate dropped into normal range, a second and more dangerous abnormal heart rhythm emerged called atrial fibrillation. Fibrillation is a term that describes a type of shivering motion of the heart muscle that does not pump blood. Instead, the blood pools and quivers. This is dangerous not only because it provides poor circulation, but also because blood will clot if it is not in motion. Atrial fibrillation is one of the main causes of embolic strokes and pulmonary embolism (clots in the lung), both which can be fatal.17 After two days, the condition did not change and the patient was cardioverted (shocked using paddles) to shock the heart back into a normal rhythm.
This was a healthy 31-year-old man, yet by taking less than 1/4mg of clenbuterol, he ended up in the hospital for four days and had to be shocked to restore a normal heartbeat. His is certainly not the only case of this drug affecting healthy young men in such a manner.10,13 In fact, this gentleman should consider himself fortunate, as others in similar situations died. The stimulatory effect of clenbuterol, said to be b2-specific, can affect the b1-receptors which control heart rate.18,19 B2-receptors also control heart rate, though this effect is minor in normal people. It is possible that b2-stimulation in a case of clenbuterol overdose contributes to tachycardia, though a recent study investigating the use of clenbuterol in acute heart failure challenges this position.20 This is particularly evident at high doses, as seen in this case. Yet, the greatest danger from clenbuterol overdose may not be the b1-stimulatory effect on the heart rate, but rather on the drug’s effect on the electrolyte balance.12,21 Electrolytes include familiar names, such as sodium, potassium, magnesium and calcium. Normally, the body maintains these electrolytes in a controlled range because they are involved in the conduction of electrical signals in the brain, nerves and heart muscle. In clenbuterol overdose, the electrolyte balance can be disturbed and electrical signals throughout the body may become abnormal. In extreme cases, this can lead to heart attacks, acute heart failure or even death.
Summarise
 Albuterol is the weaker version of Clenbuterol but with fewer side effects and with less severe side effects. Users of this drug are advised to take amino acids (especially Taurine), Omega 3, CLA, ALA, and milk thistle to prevent liver toxicity and depletion of taurine and potassium levels in the body.
Albuterol is the weaker version of Clenbuterol but with fewer side effects and with less severe side effects. Users of this drug are advised to take amino acids (especially Taurine), Omega 3, CLA, ALA, and milk thistle to prevent liver toxicity and depletion of taurine and potassium levels in the body.
A big plus is that Albuterol has the ability to increase endurance and strength besides reducing LDL (low-density lipoprotein, bad cholesterol), increasing HDL (high-density lipoprotein, good cholesterol), and reducing total cholesterol
Clenbuterol may have a negative effect on your heart and vascular system (BP) but this may be dependant on your individual tolerance. And let’s be honest all PED’s carry health risks, just like the pharmaceutical drugs your doctor is eager to prescribe.
Still if you do want to use the most healthy of these two (more analogues will follow) or if you are suffering from problems like trembling, insomnia anxiety and/or are prone to panic attacks then Albuterol is probably the better choice between the two, being the milder little brother. This is oc especially true for for people that practical “ live on it”. Like in the past on T3.