
Can We Built Muscle Without Training?

We all know that steroids are building muscles. But what is really interesting and subject of much discussion and speculation. Can we build muscles if we administer anabolic steroids as injects and orals, without training? The question then would be, how much and how long?
I n his days Arnold was what thought to be the biggest possible, he was a freak and probably the best what could happen to bodybuilding. Because he was very charismatic. What followed was an increase in gyms and gymrats, many wanted to become as big as Arnold and some wanted to become even bigger.
n his days Arnold was what thought to be the biggest possible, he was a freak and probably the best what could happen to bodybuilding. Because he was very charismatic. What followed was an increase in gyms and gymrats, many wanted to become as big as Arnold and some wanted to become even bigger.
What we see in the time line is that Arnold had a competition weight of around 235 lbs. In the Seventies Sergio Oliva was a freak at 240lbs. In the Nineties Dorian Yates was weighing 268lbs. In 2000’s Ronnie Coleman reached a competition weight of 297lbs, and now Big Ramy walked on stage at 316 lbs! Off season he reached an unbelievable 339 lbs. And he is able to keep his vascularity and lean look and, nowadays very important, he has no distended belly.
During all those years training and nutrition didn’t change that much but drug use has, and with it the increased mass/weight of the bodybuilders and other iron warriors. And it’s not only anabolic steroids anymore, lately GH, IGF-1, SARMS, insulin and peptides entered the scene. I’m not even touching SE oils etc. Just want to talk about the mere muscle builders.
Dose response Forbes
Gilbert B. Forbes in 1985 speculated that there was a linear relationship between Testosterone dose and lean mass accretion. For years, athletes and scientists have
 nonetheless disagreed about the effect of anabolic steroids on strength, muscle mass, and health status. The data from this thorough study support Forbes' assertion: weekly injections of Testosterone enanthate result in dose-dependent increases in muscle mass, muscle size, strength, and power. The downside is that HDL-C tends to take a nasty dip and at higher doses hemoglobin levels rise a smidgeon
nonetheless disagreed about the effect of anabolic steroids on strength, muscle mass, and health status. The data from this thorough study support Forbes' assertion: weekly injections of Testosterone enanthate result in dose-dependent increases in muscle mass, muscle size, strength, and power. The downside is that HDL-C tends to take a nasty dip and at higher doses hemoglobin levels rise a smidgeon
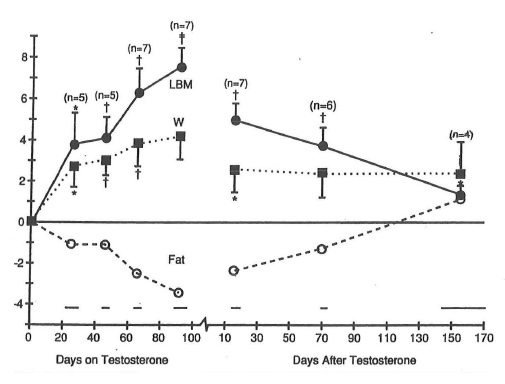 Solid evidence that these superdoses are in fact effective came from a clever retrospective study by Gilbert Forbes who suggested that the relation between lean body mass and androgen is a function of the total dosage; namely, after administration of about 10 gram exogenous androgen, lean body weight increases about 18 kg.
Solid evidence that these superdoses are in fact effective came from a clever retrospective study by Gilbert Forbes who suggested that the relation between lean body mass and androgen is a function of the total dosage; namely, after administration of about 10 gram exogenous androgen, lean body weight increases about 18 kg.
It is fascinating that 15 gram is about the amount of testosterone secreted by the human testes to carry boys through puberty (from age 11 to 18) and that the mean difference in lean body mass between men and women is around 18 kg.
Forbes et al went on to show that lean body mass does not return to baseline until 150 day after discontinuing these supraphysiological doses. The black squares W is bodyweight, the black rounds are lean body weight (LBM) and the white squares are Fat.
The Dose-Response Relationship
I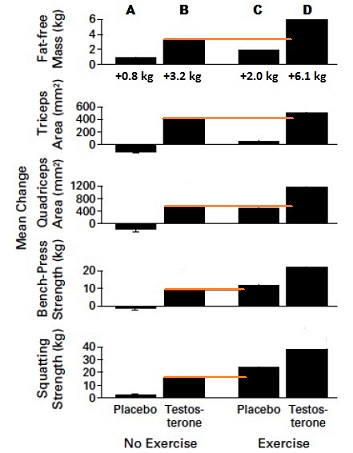 n 1996 a study from Bhasin et al, was published, that scientifically showed, what bodybuilders knew for a very long time. It showed that testosterone actually worked in building skeletal muscle (hypertrophy) and strength, it also showed that testosterone causes muscle and strength improvements even in the absence of training (B)!
n 1996 a study from Bhasin et al, was published, that scientifically showed, what bodybuilders knew for a very long time. It showed that testosterone actually worked in building skeletal muscle (hypertrophy) and strength, it also showed that testosterone causes muscle and strength improvements even in the absence of training (B)!
Over.
In this study, 43 young healthy normal weight men, were put on standardized diets and then divided into four groups:
A.No exercise, placebo
B. No exercise, 600 mg Testosterone Enanthate weekly
C. Resistance exercise 3 times per week, placebo
D. Resistance exercise 3 times per week, 600 mg Testosterone Enanthate per week for a period of 10 weeks
3.2 kg of fat free muscle mass (B) gained in 10 weeks with No exercise. Much better than the other group (C) that busted their ass in the gym. And thereby it shows, the triceps area from group B is much bigger than from group C. If it works for the triceps, it will probably work for the biceps the same. So think of it, your arms about 8 times as big with only 600 mg testosterone enanthate per week for 10 weeks, compared to the group of young healthy guys (C) working out natural!! Keeping these gains or even increase them is a whole other story. I’ll hypothesize about that at the end of this blogpost.
Shalender Bhasin’s Next Study
In 1997 Shalender Bhasin performed a new study. Being as curious as we are to the effects of AAS on muscles: “the effects of testosterone on body composition and muscle size have not been rigorously studied. The objective of this study was to determine the effects of replacement doses of testosterone on fat-free mass and muscle size in healthy hypogonadal men in the setting of controlled nutritional intake and exercise level.”
Seven hypogonadal men, 19-47 yr of age, were treated for 10 weeks with testosterone enanthate (100 mg/week) by im injections. Body weight, fat-free mass measured by underwater weighing and muscle size measured by magnetic resonance imaging were assessed before and after treatment. Energy and protein intake were standardized at 35 cal/kg.day and 1.5 g/kg.day, respectively. Body weight increased significantly from 79.2 to 83.7 after 10 weeks of testosterone replacement therapy (weight gain, 4.5 kg). Fat-free mass, measured by underwater weighing, increased from 56.0 to 60.9, but percent fat did not significantly change. The cross-sectional area of the triceps arm muscle increased from 2421 to 2721), and that of the quadriceps leg muscle increased from 7173 to 7720 mm2 , measured by magnetic resonance imaging. Muscle strength, assessed by one repetition maximum of weight-lifting exercises increased significantly after testosterone treatment.
There was no significant change in hemoglobin, hematocrit, creatinine, and transaminase levels. Replacement doses of testosterone increase fat-free mass and muscle size and strength in hypogonadal men.
And another one
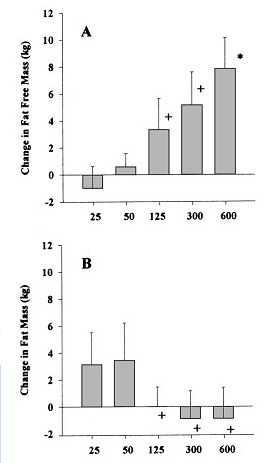
B hasin did another study (2001) in which he recruited 61 men young men (aged 18-35 )who received monthly injections of a long-acting gonadotropin-releasing hormone (GnRH) agonist to suppress endogenous testosterone secretion and weekly injections of 25, 50, 125, 300, or 600 mg testosterone enanthate/week for 20 weeks.
hasin did another study (2001) in which he recruited 61 men young men (aged 18-35 )who received monthly injections of a long-acting gonadotropin-releasing hormone (GnRH) agonist to suppress endogenous testosterone secretion and weekly injections of 25, 50, 125, 300, or 600 mg testosterone enanthate/week for 20 weeks.
Activity Control
The subjects were asked NOT to perform any type of strength training or endurance exercise during the entire study. This was done to avoid the potentially confounding influence that intense physical activity might have on the dependent variables. It is obvious that training style, volume and intensity can affect the strength results, and influence the muscle- and fat mass results. The training could also influence other endogenous anabolic hormones.
Diet Control
Two weeks before their first intramuscular injection, subjects began following a standardized diet consisting of 36 kcal/kg body weight per day (16.4 kcals/lb) and 1.2 grams protein per kilogram body weight per day (0.55 grams/lb). To put these values in perspective, a 176-pound male would have to ingest 2880 kcals/day and 96 grams of protein/day. To make sure subjects didn't change their dietary habits during the study, they were asked to complete 3-day food records and 24-hr food recalls every four weeks.
Again, consider that the normal dosage used for replacement therapy in hypogonadism is 250 mg of Test E every two to three weeks (more frequently 3 than two), i.e. 80-120 mg/week, indicating that the lowest group is probably somewhat below physiological levels, even with the administered testosterone, which shows from the figure below. The real interesting stuff is that with 600 mg/week the subjects grew 7-9 kgs of muscle (!) and lost 1-2 kgs of fat (check the table below)! That is again, without any exercise!!
tabulated results of changes in muscle mass and fat mass with hydrostatic weighing and DXA
The role of DHT
C ontext Steroid 5α-reductase inhibitors are used to treat benign prostatic hyperplasia and androgenic alopecia, but the role of 5α-dihydrotestosterone (DHT) in mediating testosterone's effects on muscle, sexual function, erythropoiesis, and other androgen-dependent processes remains poorly understood.
ontext Steroid 5α-reductase inhibitors are used to treat benign prostatic hyperplasia and androgenic alopecia, but the role of 5α-dihydrotestosterone (DHT) in mediating testosterone's effects on muscle, sexual function, erythropoiesis, and other androgen-dependent processes remains poorly understood.
Objective To determine whether testosterone's effects on muscle mass, strength, sexual function, hematocrit level, prostate volume, sebum production, and lipid levels are attenuated when its conversion to DHT is blocked by dutasteride (an inhibitor of 5α-reductase type 1 and 2).
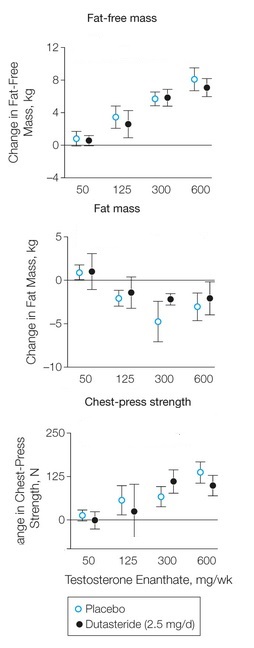 Conclusion Changes in fat-free mass in response to graded testosterone doses did not differ in men in whom DHT was suppressed by dutasteride from those treated with placebo, indicating that conversion of testosterone to DHT is not essential for mediating its anabolic effects on muscle.
Conclusion Changes in fat-free mass in response to graded testosterone doses did not differ in men in whom DHT was suppressed by dutasteride from those treated with placebo, indicating that conversion of testosterone to DHT is not essential for mediating its anabolic effects on muscle.
Although head-to-head comparisons of testosterone and DHT have not been conducted, randomized trials of DHT gel in older men have reported changes in lean body mass and in the levels of hematocrit and lipids similar to those observed in testosterone trials. Similarly, 7α-methyl 19-nortestosterone, which does not undergo 5α-reduction, maintains sexual function in hypogonadal men. These findings support the proposal that testosterone and DHT can interchangeably subserve androgen-dependent functions investigated in this trial.
The finding that 5α-reduction of testosterone to DHT is not obligatory for mediating its effects on outcomes that were studied in this trial has implications for therapeutic applications of androgens and 5α-reductase inhibitors. These findings bode well for the safety of 5α-reductase inhibitors with respect to their effects on muscle. Combined administration of testosterone plus a 5α-reductase inhibitor and the use of SARMs that do not undergo 5α-reduction have been proposed as strategies for mitigating concerns about androgen's effects on the prostate. While our data suggest that SARMs that do not undergo 5α-reduction can exert anabolic effects on the muscle, they also indicate that such a strategy may not necessarily be effective in sparing the prostate, depending upon androgen dose. The prostate safety of such SARMs will need careful scrutiny. Our data also predict that efficacy of 5α-reductase inhibitors may be limited in men with normal or high testosterone concentrations; therefore, measurement of testosterone levels might be useful in identifying men less likely to respond to 5α-reductase inhibitors.
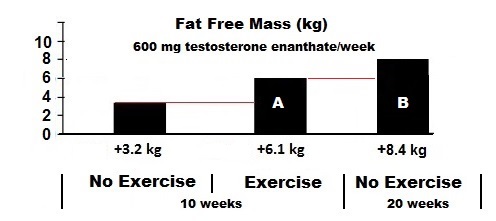
Extrapolating the information on these studies shows that 20 weeks of 600 mg/week of testosterone without training (B) still generated more lean body mass (LBM) gain than 10 weeks of steroids and training (A) above: 6.1 kg vs 8.4 kg. At the same time they lost 1-2 kg o f fat mass.
 If we compare 10 weeks of 600 mg/week testosterone enanthate (TE) no-exercise with 20 weeks of TE 600 mg/week no-exercise it shows that 10 weeks are not enough to reach full muscle growth.
If we compare 10 weeks of 600 mg/week testosterone enanthate (TE) no-exercise with 20 weeks of TE 600 mg/week no-exercise it shows that 10 weeks are not enough to reach full muscle growth.
If you can, eating maintenance dose kcals food, increase your lean body mass by 5.2 – 5.5 kg with 300 mg in 20 weeks TE per week or7.9 - 8.9 kg with 600 mg of TE per week, with no indication of saturation (biological adaption), it means that another 10 weeks could have provided more dramatic results. And I would have loved to see the same study done with 300 – 600 – 900 – 1200 mg per week for 30 weeks, because than we would probably see where saturation would take place, or gains would plateau.
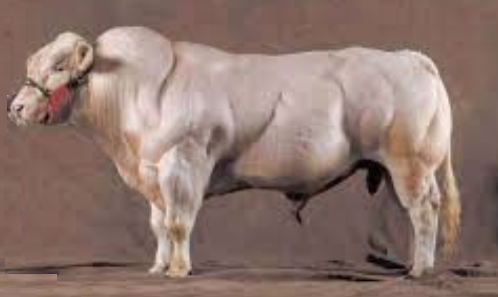
What probably fascinated me, just as other people I think, is that it is possible to loose fat and gain weight on supra-physiological doses of testosterone WITHOUT weight training or earobics. I hypotized that maybe we would be able to grow just like some of the impressive animals that never go to gym, but have enormous strength and muscle. Just think of the gorilla and the Belgian Blue. I know that the Belgian Blue is huge due to myostatin deficiency, but still. What if we would add Growth hormone, insulin and T3/T4 to the AAS cocktail in the doses the big guys use.
L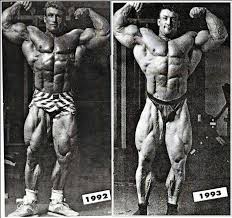 et’s look to Dorian Yates, he was one of the first bodybuilders to successfully use insulin and Growth Hormone and in about 12 month he was able to gain 30 lbs of muscle which is an absolutely insane amount for someone at his level.
et’s look to Dorian Yates, he was one of the first bodybuilders to successfully use insulin and Growth Hormone and in about 12 month he was able to gain 30 lbs of muscle which is an absolutely insane amount for someone at his level.
Truth be told most natural bodybuilders won’t gain 30 lbs of pure muscle in their whole career let alone in 12 months. Dorian likes us to believe that this change was due to his insane work ethic and modest AAS and insulin usage, but in these times of social media, the truth will always be quicker than the lie.
T hus mega-doses of AAS – GH – insulin – T3/T4 (add everything, use your imagination) and maybe some clen or ephedrine to enhance metabolism would bring us how far? And how toxic would that be?
hus mega-doses of AAS – GH – insulin – T3/T4 (add everything, use your imagination) and maybe some clen or ephedrine to enhance metabolism would bring us how far? And how toxic would that be?
After 20 weeks of 25 - 600 mg Testosterone Enanthate/week, sexual function, visual-spatial cognition, mood and PSA levels didn't change in any of the groups. None of the blood chemistry or organ toxicity values (e.g., creatinine, bilirubin, ALT, AST, etc.) were altered, with the exception of dose-dependent decreases in HDL-C that ranged from 10-20% (5-8 mg/dL), and a 9.9% increase in hemoglobin in the 600 mg group (the absolute value of 155.7 g/L was still within normal clinical limits, though).
No word of gynecomastia (gyno), shrunken testicals, female pattern fat distribution or fluid retention. How far can we go? I would like to know, but I think the ethical commissions will never agree to a study on gram doses.
