
The many faces of Trenbolone


The many faces of Trenbolone
You can find many articles on the internet about Trenbolone and mostly the writers will tell you that all Trenbolones are equel (they have the same parent compound, right?). The only difference is their half-life due to their estrification and therefore also the active compound will differ due to the molecular weight of the estrification.
Confusing, maybe but during this article I’ll try to explain clearly for all to understand.
Its not only the esterifications that are responsible for the strength effect of these copounds, but also the carriers, the solvents, co-solvents and the concentration. Where one of these Trenbolones like the Trenbolone Enanthate is effective in milligrams per millilitre, an other like Metribolone is allready active in microgrammes. Accourding to VIDA, Oral-Trenbolone (Metribolone or Methyltrienolone) has an androgenic/anabolic ratio of 6,000-7,000 /12,000-30,000 as compared to Trenbolone Acetate/Enanthate 500/ 500.
I plan to update this article on a weekly basis for a long time since I have an enormous amount of data on this subject. If aanyone wants to contribute..I'd appreciate it. You can comment here or in the forumthread on blog section
Very confusing is also that some of these compounds have different names and some people on the net just are mistaken or mixed up. Trenbolone is available as:
Trenbolone base
Like all other bases, trenbolone base has no ester. This causes a rapid release of the compound upon injection. Of course this allows the full effects of the compound to be experienced much quicker than with an estrified compound, but the same goes for the side effects. Administration of the compound and the lack of an ester requires frequent injections, most often daily or twice per day. The active life of the compound is about 24 hours. The active life highly depends on the carrier, but more about that later.
Trenbolone Acetate
Active life of this ester is about 2-3 days. Like the Trenbolone base, it must be administered frequently but this usually entails injections daily or every other day. This is probably the most popular ester of trenbolone, as the drug demands that inexperienced users administer something that can be discontinued rapidly if they react poorly. Coupled with the fact that it can be injected only every other day, it is obvious why many users prefer acetate.
Trenbolone Acetate--injectable version (Finaject and Finajet)
Trenbolone first gained fame under the brand names Finaject and Finajet, an oil based injectable veterinairy steroid containing 30milligrams per ml of trenbolone acetate. Both of these product were marketed for use in food production animals, like cattle, pigs and sheep. Numerous studies have proven the effectiviness of trenbolone, when used with an estrogen, in improving quality weight gain in these animals while they ate less grain and feed, most studies noted a significant increase in muscle size, with a decrease in fat content, imporving the "carcass quality' (meaning better steaks) in the trenbolone-treated animals.
This is correctly referred to as "Fina." Finaject is the acetate form of trenbolone. It was produced in a short acting ester (acetate), so its effect lasts only a short time and frequent administration is necessary. Finaject was an injectable steroid of veterinary medicine, which was extremely popular in bodybuilding and powerlifting during the 1980's. The injectable Trenbolone Acetate called Finaject is no longer produced.
Trenbolone Acetate--pellet form (Finaplix)
Finaplix was a veterinary cattle implant, which contained the potent androgenic steroid Trenbolone Acetate. Once Finaject and Finajet were nolonger manufactured, bodybuilders began using Finaplix to make topical or injectible versions of Trenbolone Acetate.
Today, cattle implants have become designer products with varied doses and combinations of estrogenic and/or androgenic (trenbolone) agents. So, the process of converting cattle implants to useful versions of trenbolone acetate has become more dificult since one must separate the trenbolone from the other additives present in the cattle implants before using it.
Trenbolone Hexahydrobenzylcarbonate - Trenbolone Cyclohexylmethylcarbonate – Parabolan
 Trenbolone Hexahydrobenzylcarbonate and Trenbolone Cyclohexylmethylcarbonate are exatly the same substances. Hexahydrobenzylcarbonate ester is just another name for cyclohexylmethylcarbonate ester (Its Bill Roberts that frequently used this estername when refering to Parabolan).
Trenbolone Hexahydrobenzylcarbonate and Trenbolone Cyclohexylmethylcarbonate are exatly the same substances. Hexahydrobenzylcarbonate ester is just another name for cyclohexylmethylcarbonate ester (Its Bill Roberts that frequently used this estername when refering to Parabolan).
Parabolan, was known as one of the strongest steroids available on the black market. It became harder and harder to find, until eventually it was discontinued in 1997. Negma, out of France, was the sole company who produced the anabolic steroid. Parabolan came in 1.5ml amps, and each ampule contain 76mgs of the steroid. The steroid was so popular on the black market, there were still fakes of it going around up to ten years after it was discontinued.
Once trenbolone hexahydrobenzylcarbonate was disontinued, steroid users in search of trenbolone turned to Finaject, a veterinary steroid, then to Finaplix, an implant used in cows. Users, through a process would separate the steroid from the glue and bindings, and create an injectable solution. It was often dosed at 76mgs, same as Negma's Parabolan. However, trenbolone acetate and trenbolone hexahydrobenzylcarbonate were slightly different in terms of half life. The acetate ester is much faster acting and needs to be injected, at minimum, every other day. And as powerful as trenbolone acetate is, many users who have used both trenbolone acetate and Parabolan will say the latter was much much stronger.
Today, we have trenbolone enanthate available in black markets. Trenbolone enanthate is even more comparable to trenbolone hexahydrobenzylcarbonate because it has a much longer half life and doesn't need to be injected quite as often as trenbolone acetate. Trenbolone enanthate is usually injected every 5-7 days.
Trenbolone Enanthate
As stated above it is quite similar to both Hexahydrobenzylcarbonate and Cyclohexylmethylcarbonate in terms of active life, although it is reportedly a bit longer acting. However, the major difference between enanthate and Hexahydrobenzylcarbonate and Cyclohexylmethylcarbonate is the weight of the ester. This difference is discussed below.
Metribolone – Methyltrienolone – Oral Parabolan
Accourding to VIDA, Oral Trenbolone Metribolone(Methyltrienolone) has an androgenic/anabolic ratio of 6,000-7,000/12,000-30,000 as compared to Trenbolone Acetate/Enanthate 500/500.
The effective dose of Metribolone lays between 0.1 and 1.0 mg steroid drug per day in normal adults.
Some Underground laboratories like Hard Core Labs (HCL) sell the injectable versions of oral steroids like Ana-ject, D-bol-ject and MT-DMN that contains metribolone (MT). A user was so kind to sent me his bloodvalues so we where able to compare the real bloodvalues to those many guru's like William Llewellyn expected due to scientific data. Later in this article I'll post about the bioavailability from oral vs subcutainously. //juicedmuscle.net/tags/blood-values-mt-dmn
Methyltrienolone as an orally active anabolic agent has been tested with regard to its influence on liver function. As measured by multiple parameters (BSP retention; total bilirubin; activities of transaminases, alkaline phosphatase and cholinesterase in serum; activity of proaccelerin in plasma) methyltrienolone turned out to be very active as to causing biochemical symptoms of intrahepatic cholestasis.
Kruskemper et all. Steroids. 1966 Jul;8(1):13-24
 Mixed compounds
Mixed compounds
Some UG labs ofeer mixed compounds with different length of estrifications to create stabel bloodvalues. Its comparable with Sustanon that contains 4 different esters of Testosterone.
The differences between the esters
The most important difference between the esters is wheter it is a short acting ester or a long lasting ester. The next most important difference is the weight of the ester. As mentioned under the Trenbolone Cyclohexylmethylcarbonate, the relative potency of each ester of trenbolone is partially dependent on the weight of its ester.
The half-life of a steroid ester is mostly dependent on its ratio of fat solubility to water solubility: the longer chain the ester, the higher this ratio, and the longer the half-life. In the case of Parabolan (Trenbolone cyclohexylmethylcarbonate) this carbonate ester could be most closely compared with an enanthate ester; the half-life is probably a little less than week.
The main difference between different esters is simply the number of carbon atoms in the ester. Esters and their active life are pretty much determined by the number of carbon atoms attached to a compound. Acetate has two carbon atoms, enanthate has seven, and obviously a base has no extra weight added to it. Cyclohexylmethylcarbonate is the heaviest of the esters having eight carbons attached, along with an extra oxygen. However the difference in the potency of these various esters is extremely small and should not be used to determine which product to use.
Trenbolone actate is a steroid used by farmers to improve the efficiency of meat production (muscle growth) in cattle, poultry and sheep. And it increases appetite.
Trenbolone is neither affected by aromatase or 5alpha-reductase. This means it becomes neither weaker nor stronger in androgen responsive target tissues, and is a trait usually shared by DHT (Dyhydrotestosterone) derived steroids; Since Trenbolone, it is not actually DHT derived but rather, it is derived from 19-Nor-Testosterone (Nandrolone). Trenbolone has no estrogenic activity (it may actually reduce serum estradiol levels in the body), is a very strong anabolic and androgenic compound (5x stronger than testosterone in both categories!), and it binds well to the androgen receptor. Actually, binding "well" to the androgen receptor is quite an understatement. There is no injectable AAS in our arsenal that binds to the androgen receptor (AR) as well as Trenbolone does. This is probably a major reason that Trenbolone (Parabolan) was so sought after for use as a pre-contest agent. Androgen Receptors are found in fat cells as well as muscle cells, and we all know that they act on the AR in muscle cells to promote growth, but they androgens act directly on the AR in fat cells to affect fat burning. The stronger the androgen binds to the A.R, the higher the lipolytic (fat burning) effect on adipose (fat)tissue. As if that’s not enough good news, some steroids even increase the numbers of A.R. in muscle and fat to speculate that this fat losing effect would be amplified with the concurrent use of other compounds, such as injectable testosterone. This fat burning capacity caused Trenbolone to be nicknamed as “the poor mans growth hormone”.
Another mechanism whereby Trenbolone causes muscle accumulation and fat loss is it’s ability as a nutrient partitioning agent. Basically, what this means is that while using Trenbolone, more of the food you eat will become muscle and less (if any) will become fat.
Farmers gave their livestock Trenbolone acetate due to its ability to improve feed efficiency and mineral absorption in animals, feed efficiency is a measurement of how much of an animals diet is converted into meat, the less food it takes to produce meat, the higher the efficiency.
Really, as you can see, most of Trenbolone ´s cult reputation is well deserved... And as if that’s not enough, Trenbolone noticeably increases the level of the IGF-1 within muscle tissue, which in itself is an extremely anabolic hormone. And, it’s worth noting that not only does it increase the levels of IGF-1 in muscle over two fold, it also causes muscle satellite cells (cells that repair damaged muscle) to be more sensitive to IGF-1 and other growth factors. Trenbolone ( any version) would be synergistic within a cycle containing any form of injectable IGF-1.
Trenbolone also happens to bind quite strongly to the glucocorticoid receptor as well, and this in turn imparts a nice anti-catabolic effect... which in part may help to explain why low(ish) doses of it seem to work nicely, as well as why it aids fat loss. You see, glucocorticoid hormones send a message to muscle cells to release stored protein (this is called catabolism), which is exactly the opposite of what we want.
This drug stacks well with mostly everything especially Testosterone (actually, if you want to avoid sexual dysfunction, stacking it with test is necessary). I have also found it to be a great addition to a stack containing Boldenone as well. Parabolan is most often used in cutting stacks when "quality muscle" gain is favoured over bloat and water retention.
Underground mistakes

What we see here are UG products that are degraded. This can be to various reasons. Since UG labs extracted the Trenbolone from pellets the manufacturers are used to bake their vials, after they closed them, in a a oven. If the temperature is to high the compound will degrade. Some labs are used to add the Benzyl Alcohol (BA) immediatly to the API (powder) where the BA touches the powder it will degrade the powder and later you'll notice it in the vials as dark spots. Roussel Uclaf did a lot of stability studies. I'll post a few here.
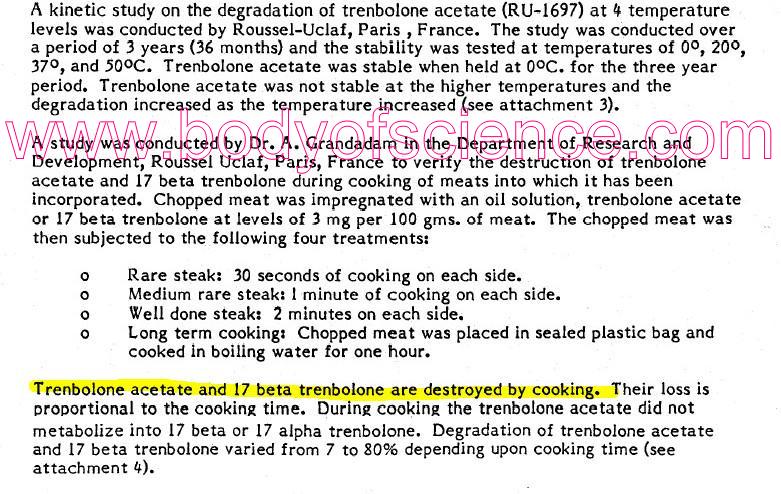
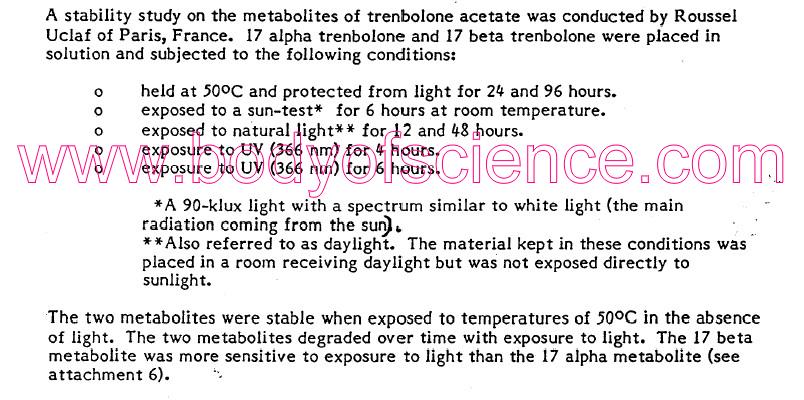
We can conclude that who is manufacturing a trenbolone product should make sure he uses not to much heat, hold his products out of the light and doesn't expose them directly to BA and other viotile co-solvents or preservatives.
Doing research for the Underground Book I visited a few UG labs. Made a pic from these small bags of Testosterone Enanthate, which melts at room temperature and slowly changes colour. This melted powder was used to colour counterfeited vials that contained further Testosterone Propionate "for the bite". Most of the buyers will never find out they used in fact a mixed Testosterone product, instead of the (pricey) Trenbolone acetate.
Side effects
Mental changes are a notorious side effect of any type of Testosterone use, and Trenbolone is no exception to this rule. Androgens increase chemicals in the brain that promote aggressive behavior, which can be beneficial for some athletes wanting to improve speed and power, but perhaps detrimental to those trying to hold a job as a social worker.
Kidney toxicity has been suggested, but has not yet been proven, and scientific evidence supporting the idea is absent from the bodybuilding community that perpetuates this idea. Early bodybuilders that used this veterinary compound and where aware of its potency, noticed the rust coloured in urine and mistook for blood. They shared it on the discussion-forums and a myth was born.
What they saw where oxidized metabolites of trenbolone, Trenbolone and 17epi-trenbolone are both excreted in urine as conjugates that can be hydrolyzed with beta-glucuronidase. This implies that trenbolone leaves the body as beta-glucuronides or sulfates.
“Trenbolone/Fina Cough”
There are two different coughs, the notorious hard and uncontrolable one that starts right after or during injection and a milder controlable one that is just irritating.
There are dozens of theories to read on the discussionforms. Most people think that if you pierce a vein or inject very close to a vein the trenbolone solution migrates up into your bloodstream and almost directly the trenbolone solution passes the lungs, an other theory is about it prostaglandins (a group of lipid cells) affecting the lungs which in turn causes a response from the bronchialis, others call it a severe allergic reaction
Most users claim that only the short estered Trenbolone acetate causes the cough, and the longer estered enanthate or hydrohexacarbenzylcarbonate (parabolan) don’t.
Personally I believe it’s the Trenbolone acetate molecule that causes the irritation in the lungs. The short esterd steroids also often cause injection pain due to their short carbon chain, simular to red ant and bee poison (propionate) and acetic acid (vinegar).
Fina-dick (Deca-dick)
Is when your penis and libido doesn't function as it normally does. Some have experienced trouble with getting an erections.
In this case your sex drive can also be inhibited. People used to stack Trenbolone with some strong androgenic steroids and/or Proviron to solve this problem. Now we we live in a time where we have access to Sildenafil (Viagra), Tadelafil or even better Vardenafil.
Recent studies that compare Trenbolone with Testosterone and SARM for HRT
17β-Hydroxyestra-4,9,11-trien-3-one (trenbolone) exhibits tissue selective anabolic activity: effects on muscle, bone, adiposity, hemoglobin, and prostate.
Yarrow JF et all. Am J Physiol Endocrinol Metab. 2011 Apr;300(4):E650-60.
Abstract
Selective androgen receptor modulators (SARMs) now under development can protect against muscle and bone loss without causing prostate growth or polycythemia. 17β-Hydroxyestra-4,9,11-trien-3-one (trenbolone), a potent testosterone analog, may have SARM-like actions because, unlike testosterone, trenbolone does not undergo tissue-specific 5α-reduction to form more potent androgens. We tested the hypothesis that trenbolone-enanthate (TREN) might prevent orchiectomy-induced losses in muscle and bone and visceral fat accumulation without increasing prostate mass or resulting in adverse hemoglobin elevations. Male F344 rats aged 3 mo underwent orchiectomy or remained intact and were administered graded doses of TREN, supraphysiological testosterone-enanthate, or vehicle for 29 days. In both intact and orchiectomized animals, all TREN doses and supraphysiological testosterone-enanthate augmented androgen-sensitive levator ani/bulbocavernosus muscle mass by 35-40% above shams (P ≤ 0.001) and produced a dose-dependent partial protection against orchiectomy-induced total and trabecular bone mineral density losses (P < 0.05) and visceral fat accumulation (P < 0.05). The lowest doses of TREN successfully maintained prostate mass and hemoglobin concentrations at sham levels in both intact and orchiectomized animals, whereas supraphysiological testosterone-enanthate and high-dose TREN elevated prostate mass by 84 and 68%, respectively (P < 0.01). In summary, low-dose administration of the non-5α-reducible androgen TREN maintains prostate mass and hemoglobin concentrations near the level of shams while producing potent myotrophic actions in skeletal muscle and partial protection against orchiectomy-induced bone loss and visceral fat accumulation. Our findings indicate that TREN has advantages over supraphysiological testosterone and supports the need for future preclinical studies examining the viability of TREN as an option for androgen replacement therapy.
********************************************
Tissue selectivity and potential clinical applications of trenbolone (17beta-hydroxyestra-4,9,11-trien-3-one): A potent anabolic steroid with reduced androgenic and estrogenic activity.
Yarrow et all, Steroids 2010 Jun;75(6):377-89.
Abstract
Recently, the development of selective androgen receptor modulators (SARMs) has been suggested as a means of combating the deleterious catabolic effects of hypogonadism, especially in skeletal muscle and bone, without inducing the undesirable androgenic effects (e.g., prostate enlargement and polycythemia) associated with testosterone administration. 17beta-Hydroxyestra-4,9,11-trien-3-one (trenbolone; 17beta-TBOH), a synthetic analog of testosterone, may be capable of inducing SARM-like effects as it binds to androgen receptors (ARs) with approximately three times the affinity of testosterone and has been shown to augment skeletal muscle mass and bone growth and reduce adiposity in a variety of mammalian species. In addition to its direct actions through ARs, 17beta-TBOH may also exert anabolic effects by altering the action of endogenous growth factors or inhibiting the action of glucocorticoids. Compared to testosterone, 17beta-TBOH appears to induce less growth in androgen-sensitive organs which highly express the 5alpha reductase enzyme (e.g., prostate tissue and accessory sex organs). The reduced androgenic effects result from the fact that 17beta-TBOH is metabolized to less potent androgens in vivo; while testosterone undergoes tissue-specific biotransformation to more potent steroids, dihydrotestosterone and 17beta-estradiol, via the 5alpha-reductase and aromatase enzymes, respectively. Thus the metabolism of 17beta-TBOH provides a basis for future research evaluating its safety and efficacy as a means of combating muscle and bone wasting conditions, obesity, and/or androgen insensitivity syndromes in humans, similar to that of other SARMs which are currently in development.
********************************************
Please keep in mind that it is done on Rats, so there is no exact medical conversion into comparable human doses without knowing the differences in metabolism/clearance of given compound/metabolites.
Mathematically, however, the conversion factor for Rat to Human is defined by the FDA to be 0.162 The conversion from Mice to Human is .081
This study does not appear to list dosages in the mg/kg range, just a total dose per Rat so we would need to figure this out.
Avg 3 month male rat weight is approx 300-500 grams. Lets just say 500 since it is easy to use 1/2 kilogram (500g) as the weight
The low dosage in the study is 1mg/week TREN per Rat, which appears to be apprx 2mg/kg/week
For a 220lb (100kg) person that equates to 200mg/week.... and then multiply by the final (Rat-Human) conversion factor of .162 and we get 32.4mg/week TREN.
Conversions for the low/med/high TREN doses in the study (rats) and approx mathematical human values:
Values for a 100kg Person via animal-human mathematical conversion
Low Dose: 32.4mg/week (Converted from 1mg/week/rat)
Med Dose: 113.4mg/week (Converted from 3.5mg/week/rat)
High Dose 226.8mg/week (Converted from 7mg/week/rat)
Anyhow, I stress that these conversions are more mathematical than medical in nature...a
Other people agree with the math above but think that the used animals weighed more in the 275-300g range. Also, please consider that they obtained a highly myotrophic effect from the "half-low" dose of TREN (0.5mg/week).
Another, perhaps more important consideration, is that FDA provides drug dose conversion factors to determine maximum recommended starting doses (MSRDs) for clinical trials based on the 'no observered adverse event level' (NOAEL) following pre-clinical toxicology studies. It's my understanding they did not perform any toxicological assessments of this agent, they simply demonstrated its myotrophic efficacy. Clearly, future pre-clinical work is required before advancing this agent to clinical testing.ure..
********************************************
- Login to post comments