
The effect of steroid esters

 Pharmacokinetics and Pharmacodynamics of Steroid Esters in Oil Vehicle:
Pharmacokinetics and Pharmacodynamics of Steroid Esters in Oil Vehicle:
Effects of Ester, Injection Site, and Injection Volume
Variations in side-chain ester chemistry are important in the pharmacokinetics of androgen esters in oil vehicle. In humans, the very short propionate (three-carbon aliphatic) ester of testosterone has distinctly shorter duration of action than esters with longer (seven- or eight-carbon) side-chains. More subtle changes in side-chain ester structure have proven ineffective in altering human clinical pharmacokinetics, because substitution of a linear aliphatic side-chain of seven carbons (enanthate) with either a saturated, cyclized, seven-carbon aliphatic chain (cyclohexanecarboxylate) or a linear, aliphatic, eight-carbon chain (cypionate) resulted in virtually unchanged kinetics. (2, 4-6, 12, 15)
Testosterone enanthate (TE) or testosterone cypionate (TC), injected intramuscularly, are the most commonly used androgen preparations with terminal half-lifes of 7-12 days. Pharmacokinetic studies indicate that the major limitations of TE and TC include relatively high peak levels and limited duration of T levels within the normal range (approximately 2 weeks), following an injection. Disadvantages of TE and TC highlighted the need for long-acting preparations of T with more stable delivery kinetics. Testosterone undecanoate (TU; 17-hydroxy-4-androsten-3-one undecanoate) is an unsaturated, aliphatic, fatty acid ester of testosterone (T) in 17β-position. In ampules containing 250 mg of the ester in 2 ml of tea seed oil in administration of 500 or 1,000 mg shows a terminal elimination half-life of 18-23 days. (4, 10, 15, 17)
 Graphic: Testosterone Cypionate. Wider variation in ester side-chain chemistry to include greater chain length and/or aromatic ring structures is a more effective determinant of ester pharmacokinetics. Nandrolone hexoxyphenylpropionate ester has far better depot properties, with a prolonged and retarded release profile, compared with the decanoate (aliphatic chain with 10 carbons). Another study indicates the decanoate (aliphatic chain with 10 carbons) ester has better depot properties than a nine-carbon chain including an aromatic ring. Because the vehicle (arachis oil) was unchanged during this latter study and because of the experimental observation that the oil vehicle influences local reaction to the oil injection, as well as androgen ester pharmacology, these conclusions may be extrapolated to other vegetable oil injection vehicles only with caution. (2, 7, 13, 14, 16)
Graphic: Testosterone Cypionate. Wider variation in ester side-chain chemistry to include greater chain length and/or aromatic ring structures is a more effective determinant of ester pharmacokinetics. Nandrolone hexoxyphenylpropionate ester has far better depot properties, with a prolonged and retarded release profile, compared with the decanoate (aliphatic chain with 10 carbons). Another study indicates the decanoate (aliphatic chain with 10 carbons) ester has better depot properties than a nine-carbon chain including an aromatic ring. Because the vehicle (arachis oil) was unchanged during this latter study and because of the experimental observation that the oil vehicle influences local reaction to the oil injection, as well as androgen ester pharmacology, these conclusions may be extrapolated to other vegetable oil injection vehicles only with caution. (2, 7, 13, 14, 16)
 Graphic: Testosterone EnanthateIn addition to the chemistry of the side-chain ester, both injection site and volume can systematically influence blood levels after intramuscular injection of esters in an oil vehicle formulation. Injection site may be important because of differences in tissue composition and blood flow. Intramuscular oil-based injections may more accurately be termed intermuscular or intralipomatous. The former reflects the tendency of oil vehicle to distribute along intermuscular fascial planes, whereas the latter depends upon the amount of fat at the injection site (including systematic gender differences) together with needle geometry and anatomy of the injection depot. Intralipomatous deposition of injections with a larger vehicle volume may explain the slower release kinetics of nandrolone decanoate in the gluteal region, as well as the differences from the deltoid site, which has a lower fat content. (1, 13)
Graphic: Testosterone EnanthateIn addition to the chemistry of the side-chain ester, both injection site and volume can systematically influence blood levels after intramuscular injection of esters in an oil vehicle formulation. Injection site may be important because of differences in tissue composition and blood flow. Intramuscular oil-based injections may more accurately be termed intermuscular or intralipomatous. The former reflects the tendency of oil vehicle to distribute along intermuscular fascial planes, whereas the latter depends upon the amount of fat at the injection site (including systematic gender differences) together with needle geometry and anatomy of the injection depot. Intralipomatous deposition of injections with a larger vehicle volume may explain the slower release kinetics of nandrolone decanoate in the gluteal region, as well as the differences from the deltoid site, which has a lower fat content. (1, 13)
Graphic: Nandrolone PhenylPropionate
.jpg) There is a rapid and dose-proportional increase in nandrolone serum levels across a dose range after a single intramuscular injection of 50–150 mg nandrolone decanoate in healthy young men with peak serum levels of nandrolone reached 2–3 d after injection. Subsequently, nandrolone levels decreased, but were still measurable 32 d after dosing in approximately half the subjects in the 50-mg group and in all subjects in the 100- and 150-mg groups. The half-life ranged from 7.1 days – 11.8 days. In addition, urinary metabolites 19-NA and/or 19-NE were detectable for up to 6 months after the 100 and 150 mg injection in a significant proportion of subjects. (2)
There is a rapid and dose-proportional increase in nandrolone serum levels across a dose range after a single intramuscular injection of 50–150 mg nandrolone decanoate in healthy young men with peak serum levels of nandrolone reached 2–3 d after injection. Subsequently, nandrolone levels decreased, but were still measurable 32 d after dosing in approximately half the subjects in the 50-mg group and in all subjects in the 100- and 150-mg groups. The half-life ranged from 7.1 days – 11.8 days. In addition, urinary metabolites 19-NA and/or 19-NE were detectable for up to 6 months after the 100 and 150 mg injection in a significant proportion of subjects. (2)
 Mean serum concentration profiles for nandrolone after single gluteal muscle injection in 1 ml arachis oil of 50, 100, or 150 mg nandrolone decanoate in healthy men.
Mean serum concentration profiles for nandrolone after single gluteal muscle injection in 1 ml arachis oil of 50, 100, or 150 mg nandrolone decanoate in healthy men.
Nandrolone displays so-called flip-flop pharmacokinetics, which means that the ascending phase of the curve represents the disposition of nandrolone and the descending part of the curve represents the rate-limiting process of release of nandrolone decanoate from the muscle into the general circulation. The half-life in the descending phase of the curve is an estimate of the absorption half-life rather than the elimination half-life. (2)
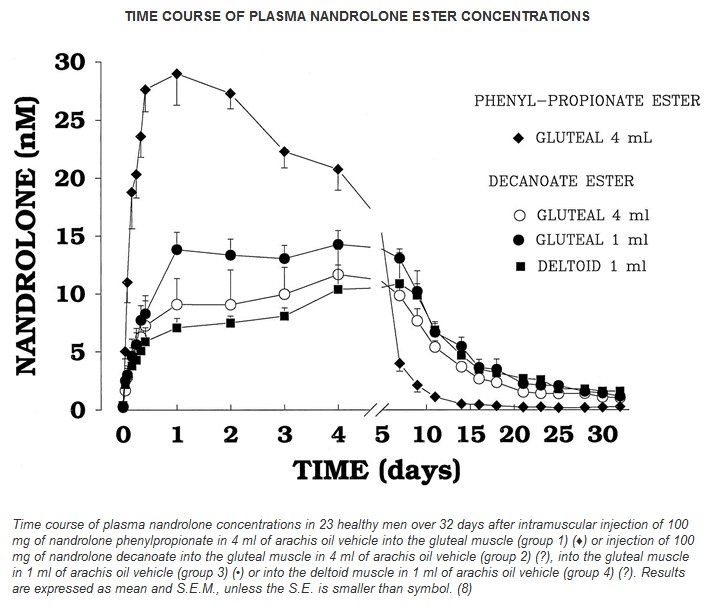
In the following study, 23 healthy men were randomized into four groups receiving a single dose of 100 mg nandrolone esters: nandrolone phenylpropionate in 4 ml arachis oil injected into the gluteal muscle (group 1), nandrolone decanoate in 4 ml arachis oil injected into the gluteal muscle (group 2), nandrolone decanoate in 1 ml arachis oil injected into the gluteal muscle (group 3), or nandrolone decanoate in 1 ml arachis oil injected into the deltoid muscle (group 4). Absolute bioavailability was higher after single-dose injection of 100 mg nandrolone decanoate in 1 ml arachis oil into the gluteal muscle (73%) than in the other three groups (53–56%). (8)

Corresponding to the patterns of blood concentrations, pharmacodynamic indices reflecting androgen-induced inhibition of pituitary-testicular function, namely blood testosterone and inhibin concentrations, are also systematically influenced by these factors. Testosterone and inhibin concentrations represent effective markers of endogenous pituitary gonadotropin (LH and FSH, respectively) secretion. This reflects the physiological fact that pituitary LH acts exclusively upon testicular Leydig cells, due to their unique expression of cell surface membrane LH receptors. In healthy men, virtually all circulating testosterone originates from Leydig cells, with an absolute requirement for trophic influence from LH derived from the bloodstream. Similarly, pituitary FSH acts exclusively upon testicular Sertoli cells, which uniquely express FSH receptors on their cell surface membranes, and virtually all circulating immunoreactive inhibin originates from the gonads. As a result, blood levels of these two hormones are useful integrated bioassay indicators of endogenous pituitary gonadotropin secretion, as reflected by the testicular hormonal response to ambient blood LH and FSH levels. These two pharmacodynamic indices show physiologically meaningful distinctions between the esters and the effects of injection site and volume. (8, 9, 11)
The pharmacodynamic variability in plasma testosterone and inhibin concentrations is accounted for by the variability between esters and the site and volume of injection of the nandrolone injections. The overall kinetics of suppression of testosterone is dominated by the slow negative feedback system, rather than the much faster metabolic clearance of testosterone. This negative feedback is mediated via inhibition of pulsatile gonadotropin-releasing hormone secretion from hypothalamic neurons into the pituitary portal system and then pituitary LH secretion from gonadotropes. This is in stark contrast to a highly potent and specific gonadotropin-releasing hormone antagonist that causes immediate cessation of gonadotropin-releasing hormone action leading to castrate testosterone concentrations within 12 hr, compared with 5 to 10 days with AAS administration. After a single 100 mg injection of NPP, recovery takes 10+ days. After ND, recovery takes 15+ days. It is important to note these are single administrations of 100 mg. HPTA recovery with repeated doses of 200+ mg is long!!!! (3, 8)
Administration of androgens such as testosterone and 19-nor-testosterone has been most frequently via depot intramuscular injections of steroid esters dissolved in a vegetable oil vehicle. Intramuscular injections provide sustained androgen release into the circulation and remain the mainstay of androgen replacement therapy. Experimental studies suggest that absorption rates are predicted by the oil/water partition coefficients (or hydrophobicity) and that the oil vehicle is absorbed more slowly than the androgen ester, with gradual release into the extracellular fluid, where esters are rapidly hydrolyzed to liberate biologically active steroid. As the above shows, other factors influence steroid appearance in the bloodstream that include the chemistry of the side-chain ester (hydrophobicity, steric hindrance of hydrolysis, and solubility), as well as injection factors (technique, depth, site, volume, Ph, and osmolarity of the solution).
1. Al-Hindawi MK, James KC, Nicholls PJ. Influence of solvent on the availability of testosterone propionate from oily, intramuscular injections in the rat. J Pharm Pharmacol 1987;39(2):90-5.
2. Bagchus WM, Smeets JMW, Verheul HAM, De Jager-Van Der Veen SM, Port A, Geurts TBP. Pharmacokinetic Evaluation of Three Different Intramuscular Doses of Nandrolone Decanoate: Analysis of Serum and Urine Samples in Healthy Men. J Clin Endocrinol Metab 2005;90(5):2624-30.
3. Behre HM, Klein B, Steinmeyer E, McGregor GP, Voigt K, Nieschlag E. Effective suppression of luteinizing hormone and testosterone by single doses of the new gonadotropin-releasing hormone antagonist cetrorelix (SB-75) in normal men. J Clin Endocrinol Metab 1992;75(2):393-8.
4. Behre HM, Nieschlag E. Testosterone buciclate (20 Aet-1) in hypogonadal men: pharmacokinetics and pharmacodynamics of the new long-acting androgen ester. J Clin Endocrinol Metab 1992;75(5):1204-10.
5. Belkien L, Schurmeyer T, Hano R, Gunnarsson PO, Nieschlag E. Pharmacokinetics of 19-nortestosterone esters in normal men. J Steroid Biochem 1985;22(5):623-9.
6. Fujioka M, Shinohara Y, Baba S, Irie M, Inoue K. Pharmacokinetic Properties of Testosterone Propionate in Normal Men. J Clin Endocrinol Metab 1986;63(6):1361-4.
7. Khankhanian NK, Hammers YA, Kowalski P. Exuberant local tissue reaction to intramuscular injection of nandrolone decanoate (Deca-Durabolin)–a steroid compound in a sesame seed oil base–mimicking soft tissue malignant tumors: a case report and review of the literature. Mil Med 1992;157(12):670-4.
8. Minto CF, Howe C, Wishart S, Conway AJ, Handelsman DJ. Pharmacokinetics and pharmacodynamics of nandrolone esters in oil vehicle: effects of ester, injection site and injection volume. J Pharmacol Exp Ther 1997;281(1):93-102.
9. Nieschlag E, Cuppers HJ, Wiegelmann W, Wickings EJ. Bioavailability and LH-suppressing effect of different testosterone preparations in normal and hypogonadal men. Horm Res 1976;7(3):138-45.
10. Schubert M, Minnemann T, Hubler D, et al. Intramuscular testosterone undecanoate: pharmacokinetic aspects of a novel testosterone formulation during long-term treatment of men with hypogonadism. J Clin Endocrinol Metab 2004;89(11):5429-34.
11. Schulte-Beerbuhl M, Nieschlag E. Comparison of testosterone, dihydrotestosterone, luteinizing hormone, and follicle-stimulating hormone in serum after injection of testosterone enanthate of testosterone cypionate. Fertil Steril 1980;33(2):201-3.
12. Schurmeyer T, Nieschlag E. Comparative pharmacokinetics of testosterone enanthate and testosterone cyclohexanecarboxylate as assessed by serum and salivary testosterone levels in normal men. Int J Androl 1984;7(3):181-7.
13. Tanaka T, Kobayashi H, Okumura K, Muranishi S, Sezaki H. Intramuscular absorption of drugs from oily solutions in the rat. Chem Pharm Bull (Tokyo) 1974;22(6):1275-84.
14. van der Vies J. Implications of basic pharmacology in the therapy with esters of nandrolone. Acta Endocrinol Suppl (Copenh) 1985;271:38-44.
15. Weinbauer GF, Partsch C-J, Zitzmann M, Schlatt S, Nieschlag E. Pharmacokinetics and Degree of Aromatization Rather Than Total Dose of Different Preparations Determine the Effects of Testosterone: A Nonhuman Primate Study in Macaca fascicularis. J Androl 2003;24(5):765-74.
16. Wijnand HP, Bosch AM, Donker CW. Pharmacokinetic parameters of nandrolone (19-nortestosterone) after intramuscular administration of nandrolone decanoate (Deca-Durabolin) to healthy volunteers. Acta Endocrinol Suppl (Copenh) 1985;271:19-30.
17. Zhang GY, Gu YQ, Wang XH, Cui YG, Bremner WJ. A pharmacokinetic study of injectable testosterone undecanoate in hypogonadal men. J Androl 1998;19(6):761-8.
--------------------------------------------------------------------------------
- Login to post comments